Can Straining on the Toilet Cause a Stroke in Older Adults? A TCM Look at Four Hidden Risks of Chronic Constipation
"Grandpa fainted in the bathroom last night" is not an isolated case. Straining on the toilet can indeed trigger strokes and heart attacks in older adults — but that is only one of four hidden risks of long-term constipation. This guide unpacks the four: cardiovascular events from straining, chronic blood loss from haemorrhoids and fissures, faecal impaction with bowel obstruction, and constipation masking colorectal cancer warning signs. It lists when to seek immediate medical attention, the age range for Hong Kong's colorectal cancer screening programme, and the TCM view of common patterns and direction.
Medical review: Dr. Chan Wing Kiu, Joanne,Registered Chinese Medicine Practitioner #009463
1-Minute Quick Answer
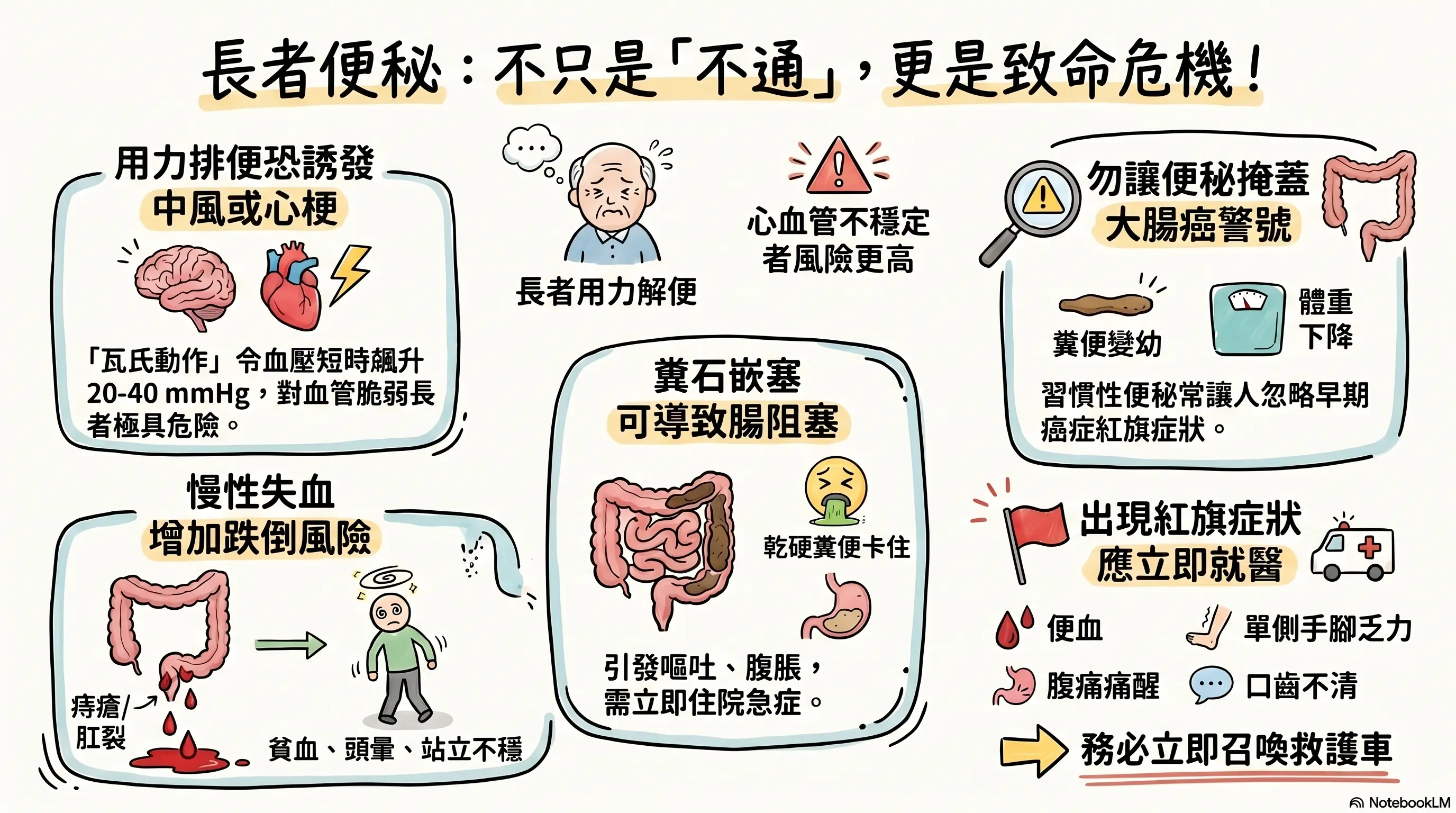
Straining on the toilet can genuinely trigger a stroke or cardiac event in older adults via the Valsalva manoeuvre's sharp blood-pressure spike. Chronic constipation carries three more risks: chronic blood loss from haemorrhoids, faecal impaction with bowel obstruction, and masking colorectal cancer signs. Blood in stool, thinner stools or a new change in bowel habits need Western assessment first. Reviewed by Dr Chan (CMCHK 009463).
Can Straining on the Toilet Cause a Stroke in Older Adults? A TCM Look at Four Hidden Risks of Chronic Constipation
 For quick reference, this image was generated by NotebookLM. Some Chinese characters may not render perfectly; we appreciate your understanding.
For quick reference, this image was generated by NotebookLM. Some Chinese characters may not render perfectly; we appreciate your understanding.
Medical review: Dr Chan Wing-kiu (CMCHK 009463; geriatric gynaecology, internal medicine)
"Grandpa was on the toilet for ages last night, didn't answer when we knocked — turned out he had fainted."
"Grandma hadn't passed stool for days; the moment she strained, her chest hurt; A&E said it was a minor cardiac event."
These cases are not rare in clinic. Strokes and heart attacks triggered by straining on the toilet have a clear physiological basis — they are not a folk scare story.
The impact of long-term constipation on older adults goes well beyond "discomfort". This article unpacks four hidden risks, lists when to seek immediate medical attention or A&E, sets out the age range and timing of Hong Kong's colorectal cancer screening programme, and adds the TCM view of common constitutional patterns.
Position: If an older adult shows blood in stool, distinctly thinner stools, unexplained weight loss, anaemia, nighttime abdominal pain, a new change in bowel habits, sudden chest pain or headache, slurred speech or one-sided weakness, call an ambulance or go straight to A&E — do not wait for a TCM assessment.
Risk 1: Straining Triggers Cardiovascular Events
When older adults strain to pass stool, they perform what medicine calls the Valsalva manoeuvre — holding the breath, tensing the abdominal muscles, raising intrathoracic pressure. For young, healthy adults this is harmless; for cardiovascularly fragile older adults it can trigger serious events.
The Valsalva manoeuvre causes:
- Brief blood-pressure spike: BP can jump 20–40 mmHg during straining
- Heart-rate changes: rate may drop suddenly or become irregular
- Altered venous return: raised intrathoracic pressure temporarily blocks venous return; once straining ends, blood floods back, hitting the heart again
- Raised intracranial pressure: greatest risk for older adults with cerebral aneurysm, uncontrolled severe hypertension or carotid stenosis
High-risk groups:
- Coronary artery disease, heart failure, arrhythmia
- Uncontrolled hypertension (especially ≥ 160/100 mmHg)
- Prior stroke or cerebral aneurysm
- Aortic aneurysm
- Severe anaemia
In short, the more cardiovascularly unstable the older adult, the higher the risk from straining. With any of the above history, constipation is not just a "bowel issue" — overall strategy must be discussed with the family doctor or cardiologist.
Risk 2: Haemorrhoids, Anal Fissures and Chronic Blood Loss
In older adults with long-term constipation, hard stools and excessive straining commonly damage anal tissue, leading to haemorrhoids and fissures. This may seem minor, but clinically it can develop into:
- Slight bleeding at each defecation; daily loss is small but months of it can cause chronic anaemia
- Anaemia worsens existing cardiac strain, causing breathlessness and dizziness
- Easier to faint when standing — falls risk rises markedly
- Some older adults hold in stools to avoid pain, making constipation worse — a vicious cycle
Importantly, not all rectal bleeding is haemorrhoids. Dark-red blood, mucus, or blood streaks on the surface (rather than dripping) may indicate a problem higher in the bowel (including colorectal cancer) — never self-diagnose as "just haemorrhoids". Any new rectal bleeding in an older adult warrants assessment by a family doctor or gastroenterologist.
Risk 3: Faecal Impaction and Bowel Obstruction
In severely constipated older adults — especially the higher-risk groups below — faecal impaction can develop, where a large hard stool mass becomes stuck in the rectum or sigmoid colon:
- Patients with dementia (forget to go, blunted sensation)
- Long-term bedridden or very low-mobility patients
- On multiple constipation-inducing medications (opioid analgesics, certain antidepressants, calcium and iron supplements, certain antihypertensives)
- Post-stroke patients with swallowing difficulty and inadequate fluid intake
- Neurological diseases such as Parkinson's
Severe impaction can progress to bowel obstruction — abdominal distension, vomiting, no passage of stool or gas — an emergency requiring immediate admission. In the worst cases, it can cause bowel ischaemia, perforation and threat to life. Any older adult with no stool for 3–5 days plus distension, vomiting and significant abdominal pain must go to hospital immediately, not be given laxatives or enemas at home.
Risk 4: Constipation Masking Colorectal Cancer Warning Signs
This is the most overlooked risk. Older adults used to "passing stool every few days" may dismiss early colorectal cancer warning signs as "just worse constipation" and delay seeking care.
Red flags requiring vigilance:
- New change in bowel habits (sudden shift from constipation to diarrhoea or vice versa)
- Distinctly thinner stools, pencil-like
- Blood, mucus or pus in stool
- Unexplained weight loss (≥ 5% in 6 months)
- Persistent abdominal pain, especially waking from pain at night
- Anaemia with fatigue, pale complexion
- Sense of incomplete emptying after defecation
Hong Kong's Department of Health Colorectal Cancer Screening Programme subsidises a stool occult-blood test every 2 years for residents aged 50 to 75. With a family history or any of the red flags above, discuss earlier or more frequent colonoscopy with the family doctor. For a constipated older adult with new symptoms, the first step is always to rule out malignancy, then talk about TCM care.
When to Seek Western Care or A&E Immediately
These should not wait for a TCM assessment:
- ≥ 3 days with no passage of stool or gas, plus distension, vomiting and significant pain
- Rectal bleeding (bright red, dark red or tarry black all need investigation)
- Unexplained weight loss ≥ 5% (within 6 months)
- New change in bowel habits persisting > 2 weeks
- Distinctly thinner stools, pencil-like
- Persistent abdominal pain, waking from pain at night
- During or after defecation: sudden chest pain, breathlessness, headache, fainting, one-sided weakness, slurred speech
- Older adult with anaemia plus fatigue and pallor
In short, constipation plus any red flag warrants assessment by a family doctor or gastroenterologist first. TCM care comes in only after malignancy and emergencies have been ruled out.
How TCM Helps: Common Constitutional Patterns
In TCM, constipation in older adults is not a single pattern. Clinically common models below — for orientation only; actual differentiation requires a registered TCM practitioner reviewing tongue, pulse and overall picture.
| Constitution | Common features | Tongue | TCM direction |
|---|---|---|---|
| Fluid deficiency | Hard pellet-like stools, dry mouth, pale and dry complexion | Red tongue with scant coating | Nourish yin, moisten the bowels |
| Spleen-qi deficiency | Urge present but unable to pass; fatigue and breathlessness after straining | Pale tongue with teeth marks | Strengthen spleen, boost qi |
| Spleen-and-kidney yang deficiency | Several days without stool, cold sensitivity, sore lower back, frequent night urination | Pale plump tongue, white coating | Warm and tonify spleen and kidneys |
| Liver-qi stagnation | Irregular bowels, abdominal distension, worsens under stress | Red on the sides, thin coating | Soothe the liver, regulate qi |
Mixed presentations are more common — spleen-and-kidney yang deficiency overlaid with fluid deficiency, or spleen deficiency overlaid with liver stagnation. Prescriptions must be weighed against medications, constitution and coexisting conditions; do not self-purchase off-the-shelf "bowel-moving" Chinese patent medicines.
Five Things to Try at Home First
- 1,500–2,000 ml of fluid daily (unless under heart-failure or renal-failure fluid-restriction orders). Older adults' thirst signal is weak — prompt them in small amounts throughout the day.
- Keep a portion of fibre at each meal: leafy greens, gourds, legumes, oats. Discuss fibre supplements (psyllium husk) with the family doctor first as some medications are affected.
- 30 minutes of activity daily: stairs, walking, simple stretching all help peristalsis; bedridden patients can do in-bed leg exercises.
- Fixed toilet time: 15–30 minutes after breakfast is the strongest gastrocolic-reflex window — sit on the toilet for 5–10 minutes at the same time each day, even without urge, to build a rhythm.
- Reduce straining posture: a small footstool that raises knees above hips mimics squatting and reduces straining; never hold breath and strain hard for prolonged periods.
What Aspira TCM Clinic Looks at on Assessment
Dr Chan will work through:
- Bowel diary (frequency, shape, blood or mucus, straining required, time taken)
- Existing Western reports (occult blood, colonoscopy, CBC, renal function)
- Complete medication list (analgesics, antihypertensives, iron, calcium, antidepressants, current laxative use)
- Dietary structure, fluid intake, activity level
- Coexisting conditions (cardiovascular, diabetes, neurological disease, dementia)
- Tongue, pulse, overall constitution
Where any red flag is found, the recommendation will be to see a family doctor or gastroenterologist for occult blood or colonoscopy first, and then return for integrated care.
FAQ | Risks and Care for Constipation in Older Adults
Q1: How often per week is "normal" for an older adult?
The medical "normal" is wide — anywhere from three times a day to three times a week. What matters is not the count but whether straining is needed, whether stools are hard, and whether there is bleeding or change. A previously regular older adult whose frequency suddenly shifts for over 2 weeks should see a family doctor.
Q2: Is long-term laxative use a problem?
Depends on type. Bulk-forming laxatives (e.g. psyllium) and osmotic laxatives (e.g. lactulose) are relatively safe long term; stimulant laxatives (containing senna, aloe, phenolphthalein) can lead to bowel dependence, melanosis coli and electrolyte disturbance. Some "natural laxative teas" actually contain stimulants. Any long-term laxative use should be reviewed by the family doctor.
Q3: When should constipation prompt a colonoscopy?
Family history of colorectal cancer; a new change in bowel habits over 2 weeks; rectal bleeding; thinner stools; unexplained weight loss; anaemia — any one of these should prompt a colonoscopy discussion with the family doctor. Hong Kong residents aged 50–75 can join the Colorectal Cancer Screening Programme. Without these warning signs, the family doctor decides based on overall risk.
Q4: How should constipation in a bedridden older adult be managed?
A combination strategy is needed: regular turning, in-bed leg exercises, daily fluid tracking, scheduled toilet time (with assistance if needed), and laxatives or stool softeners as advised by the medical team. Any bedridden adult with no stool for 3–5 days plus distension and vomiting must go to hospital immediately — do not give large doses of laxatives or enemas at home, as electrolyte disturbance or perforation can result.
Q5: What about constipation in older adults on blood thinners?
For patients on warfarin or new oral anticoagulants, constipation needs special care: avoid straining (highest risk); avoid Chinese herbs that may interact with anticoagulants (such as danshen, hong hua, dang gui and other blood-moving herbs); avoid bleeding-prone approaches (stimulant laxatives may worsen haemorrhoid bleeding). Strategy should be coordinated between the family doctor and a registered TCM practitioner; bring the full medication list to follow-up.
Disclaimer: This article is for general health education only and does not replace individual diagnosis, investigation, medication or treatment. If the older adult has cardiovascular, diabetic, chronic kidney, dementia or gastrointestinal disease, follow doctors' instructions for follow-up; any laxative, herbal or supplement change should be discussed with the treating doctor first.
Disclaimer: This article is for health education and reference purposes only and does not constitute medical advice, diagnosis, or treatment. Each patient's condition is unique and treatment outcomes vary. Please consult a registered TCM practitioner or qualified healthcare professional for health concerns.
Want to learn more? WhatsApp us for a free consultation
Book via WhatsAppExplore our full range of treatments: Traditional TCM Services
Related Articles

Do Oysters, Maca and Deer Antler Boost Male Vitality? 5 Myths
Do aphrodisiac foods actually work? This article opens with a rating table (effective / partly effective / effective within a TCM framework / weak evidence / no strong evidence), reviews the Chinese and Western medical evidence behind oysters, maca, deer antler, sea cucumber and Chinese chives, distils the 3 shared traits of foods that genuinely support male sexual function, and flags 3 commonly eaten items that can actually harm performance.

Male Menopause Through the TCM Lens: 5 Signs in Men Over 40
Unexplained fatigue, irritability, lower libido, poorer sleep and a growing belly after 40 are not just ageing or work stress — they may be male menopause. This article begins with a five-sign self-check, sets out three TCM patterns (kidney-yang deficiency, kidney-yin deficiency, liver-and-kidney insufficiency) with matching improvements, and compares the two treatment routes — testosterone replacement therapy versus TCM constitutional care.
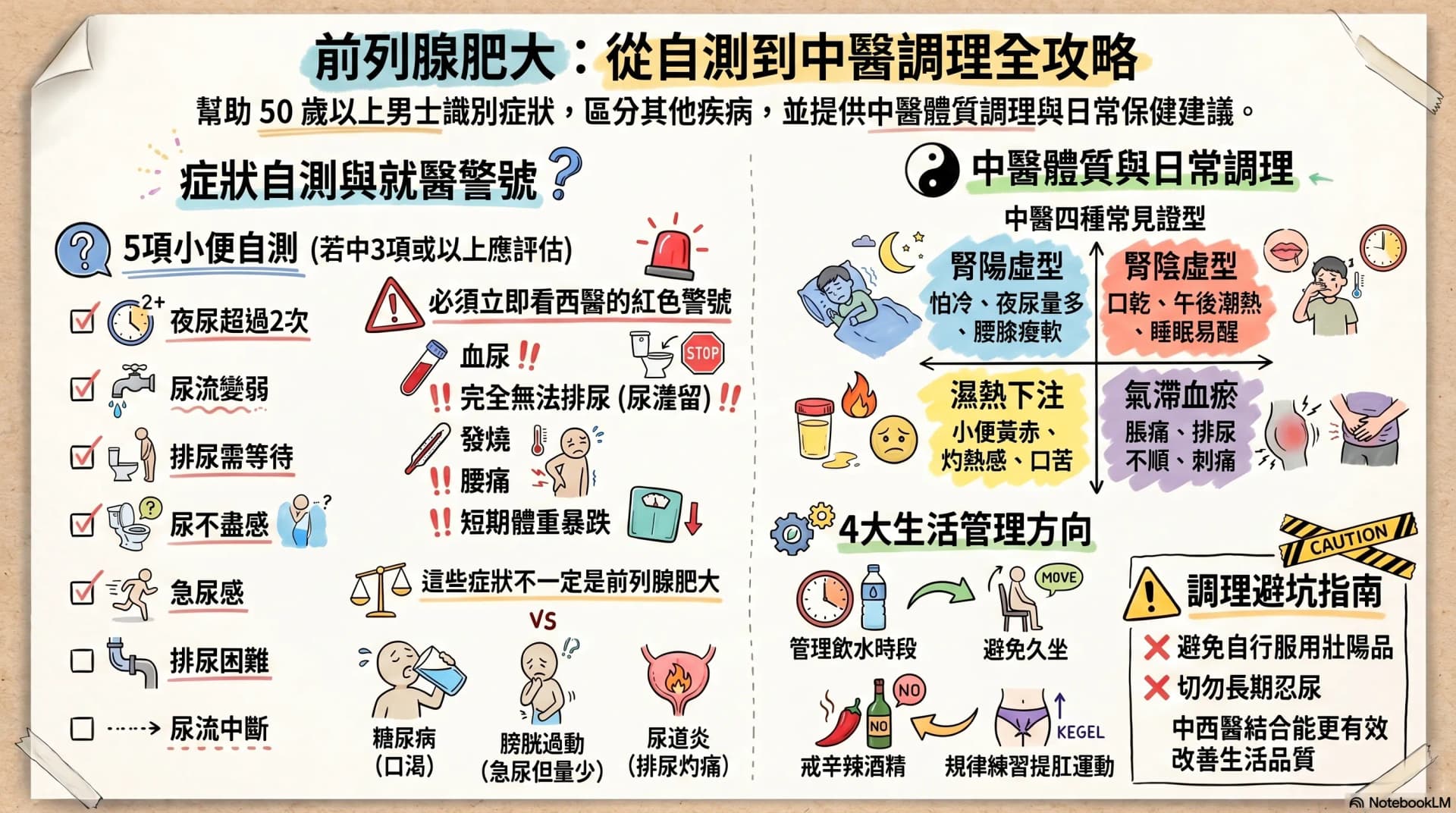
Enlarged Prostate: Are Nocturia and a Weak Stream Warning Signs?
After age 50, urinary frequency, nocturia, a weaker stream and having to urinate in stages may not simply be ageing. This article opens with a 7-symptom self-check, then sets out warning signs that warrant seeing a Western doctor immediately, four TCM constitution patterns, and four daily care directions any man can start with — helping you or your father decide the next step.