Considering Acupuncture After a Stroke? A TCM Guide to the Golden-Window Timing and Five Things Families Must Know
A family member has just been discharged after a stroke; one side is still weak and speech is slurred. The children want to start TCM acupuncture as soon as possible — but worry about interactions with blood thinners, conflicts with physiotherapy, and whether the "golden window" must be hit. This guide unpacks the meaning of the post-stroke golden-window timeline, lists the five recurrence warning signs that families must address before acupuncture begins, the logic of point selection and treatment direction, four common TCM patterns, contraindications and how to divide work with the Western rehab team.
Medical review: Dr. Chan Wing Kiu, Joanne,Registered Chinese Medicine Practitioner #009463
1-Minute Quick Answer
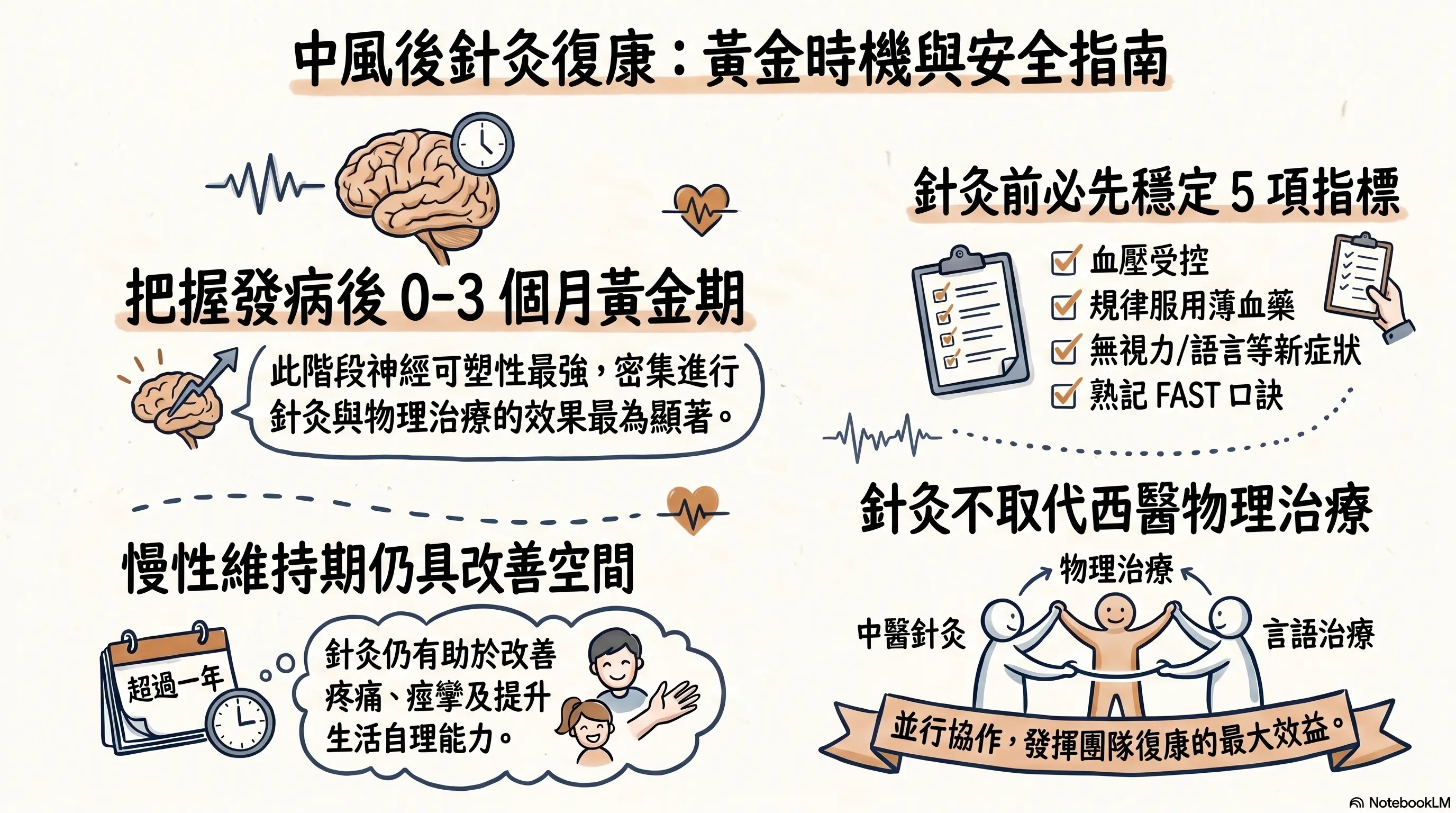
The first 0 to 3 months after a stroke is when neuroplasticity peaks and rehab works best, but "once the golden window passes there is no point" is not true — gains remain possible at 6 to 12 months. Before acupuncture begins, families must confirm five things are stable, including blood pressure, blood sugar and blood-thinner adherence, and learn FAST. Acupuncture runs alongside physiotherapy and speech therapy, not in place of Western rehab. Any new symptom needs immediate hospital care. Reviewed by Dr Chan (CMCHK 009463).
Considering Acupuncture After a Stroke? A TCM Guide to the Golden-Window Timing and Five Things Families Must Know
 For quick reference, this image was generated by NotebookLM. Some Chinese characters may not render perfectly; we appreciate your understanding.
For quick reference, this image was generated by NotebookLM. Some Chinese characters may not render perfectly; we appreciate your understanding.
Medical review: Dr Chan Wing-kiu (CMCHK 009463; geriatric gynaecology, internal medicine)
"Three months ago Dad suddenly lost movement on his left side and slurred his speech — A&E saved him. Neurology says he's stable now and can start rehab. I've heard TCM acupuncture is good for stroke — should we start as early as possible? Will it interfere with the blood thinners he's on?"
"Mum has been out of hospital for six months — her left hand still can't lift heavy things and she needs help walking. People say 'once the golden window passes there's no point' — is acupuncture still worth doing?"
"The physiotherapist's waiting list is two months. Can we do TCM acupuncture first? Will the two conflict?"
These are common questions from stroke families. TCM acupuncture has a clear role in post-stroke rehab, but timing, safety prerequisites and division of work with the Western rehab team — none of these can be skipped. Blindly "as early as possible" or "as much as possible" can expose patients to unnecessary risk.
This article unpacks the meaning of the golden-window timeline, lists the five recurrence warning signs families must address before acupuncture begins, four common TCM patterns, contraindications, and how to divide work with the Western rehab team.
Position: Stroke is an emergency. Any suspected stroke symptoms (FAST: Face droop, Arm weakness, Speech slurred, Time to call an ambulance) must trigger an immediate ambulance call to A&E — do not wait for a TCM assessment. The TCM role is to complement after acute-phase stabilisation, working alongside neurology rehab — never replacing Western treatment, medication or rehab plans.
What Is the Post-Stroke Golden Window?
The nervous system has a degree of plasticity after stroke; clinically there is a "golden window" concept:
- 0 to 3 months post-stroke: peak plasticity; intensive rehab (physiotherapy, occupational therapy, speech therapy, acupuncture) shows the strongest effect
- 3 to 6 months: meaningful functional gains still possible; intensive rehab continues
- 6 to 12 months: pace slows but maintenance and small gains remain possible
- Beyond 1 year: maintenance phase — focus shifts to preventing decline and complications (joint contracture, muscle atrophy, falls)
"Once the window passes there's no point" is not entirely true — acupuncture, physiotherapy and home exercise in the maintenance phase still contribute on pain, spasticity, balance and self-care. But the first 3 months is genuinely when intervention shows the strongest impact.
If a family member has just been discharged and neurology has confirmed stability, the earlier you discuss with a registered TCM practitioner and physiotherapy team, the better the typical results.
Five Things Families Must Know Before Acupuncture Begins
Before TCM acupuncture starts, all five of the following must be confirmed stable with neurology:
First, blood-pressure control. Uncontrolled hypertension is the single biggest stroke-recurrence risk factor. The household should have a habit of self-measuring; targets are typically below 140/90 mmHg, with the specific target set by neurology or the family doctor. If BP is swinging or above the warning line, hold acupuncture and address BP first.
Second, blood-glucose control. Diabetic and prediabetic patients have markedly higher recurrence risk. Fasting glucose, HbA1c and daily glucose checks should follow doctor's instructions.
Third, antiplatelet/anticoagulant adherence. Acute ischaemic stroke patients usually need long-term antiplatelet medication (such as aspirin, clopidogrel) or new oral anticoagulants; atrial-fibrillation strokes typically require warfarin or new oral anticoagulants. Never stop or reduce dosage on your own — any change must come from neurology. Bring a complete medication list to the first acupuncture visit; the registered TCM practitioner will adjust technique and point selection based on bleeding risk.
Fourth, return to A&E for any new symptoms. Any new weakness, slurred speech, facial droop, severe headache, vomiting, sudden vision change, sudden balance loss or cognitive confusion must trigger an immediate hospital visit — do not wait for the next follow-up or for a TCM assessment.
Fifth, master FAST. The household should know the FAST mnemonic (Face droop, Arm weakness, Speech slurred, Time to call) and post it visibly. It applies to other older adults in the household too.
If any one of these five is not in place, hold off on acupuncture and stabilise with neurology first.
How Acupuncture Is Introduced: Logic and Direction
When neurology has confirmed stability and the five items are addressed, the registered TCM practitioner will work through:
- History and medication-list review (antihypertensives, antiplatelets/anticoagulants, glucose-lowering, lipid-lowering)
- TCM four diagnostics: complexion, tongue, pulse, overall vitality
- Initial assessment of affected-side strength, sensory abnormality, range of motion
- Initial screen of speech and swallowing
- Cognitive function and mood (post-stroke depression is not uncommon)
Point-selection logic (no specific prescriptions given here) typically includes:
- Scalp acupuncture: stimulation of areas projecting to the motor cortex, supporting affected-limb movement
- Body acupuncture: predominantly the affected side's hand and foot yang channels; combining proximal and distal points
- Speech-related points: matched to the degree of dysarthria
- Swallowing-related points: where dysphagia is present (dysphagia is high-risk and must be assessed first by a speech therapist)
Frequency and treatment length vary per patient. Coordination among the family doctor or neurology, the registered TCM practitioner and the physiotherapist is recommended to avoid fatigue. Actual prescriptions are decided by the registered TCM practitioner on individual assessment; this article does not provide a uniform frequency recommendation.
TCM View of Post-Stroke Sequelae: Four Common Patterns
In TCM, the core pathogenesis of post-stroke sequelae commonly involves the directions below. The table is for orientation only; actual differentiation requires a registered TCM practitioner reviewing tongue, pulse, full symptoms, imaging and medications.
| Pattern | Common features | TCM direction |
|---|---|---|
| Qi deficiency with blood stasis | Marked weakness on the affected side, dull complexion, purplish tongue | Boost qi, move blood, resolve stasis, open channels |
| Phlegm-damp obstructing the channels | Stiff affected side, slurred speech, thick white tongue coating | Transform phlegm, open channels, strengthen spleen |
| Liver and kidney depletion | Longer course; with dizziness, tinnitus, sore lower back and knees | Tonify liver and kidney, nourish yin, anchor yang |
| Wind-phlegm-stasis obstruction | Occasional facial droop or drooling persisting after the acute phase | Extinguish wind, transform phlegm, move blood |
Mixed patterns are common in clinic and shift as recovery progresses. The same patient may move from one pattern to another over time, with the direction adjusted accordingly.
When Acupuncture Is Not Suitable or Should Be Held
- Fever, acute infection (including urinary infection, pneumonia)
- Skin ulcers, severe rash, infection
- Low platelets (< 50,000/μL) or coagulopathy
- On warfarin with INR above the therapeutic range
- Patient strongly refusing or unable to lie still
- Unstable heart rate (uncontrolled atrial fibrillation, especially new-onset or poorly controlled)
- Acute phase (within one week of stroke) — generally not recommended; decision rests with neurology
- Severe cognitive impairment unable to express discomfort
How to Divide Work with the Western Rehab Team
Post-stroke rehab is teamwork — no single profession can do it all:
| Role | Main responsibility |
|---|---|
| Neurologist | Recurrence-risk assessment, medication adjustment, imaging follow-up |
| Physiotherapist | Gait, strength, balance, spasticity management |
| Occupational therapist | ADL function, home assessment, assistive devices |
| Speech therapist | Dysarthria, swallowing training |
| Registered TCM practitioner | Constitutional care, acupuncture (motor / speech / swallowing related) |
| Psychology / psychiatry | Post-stroke depression, anxiety, cognition |
TCM acupuncture does not replace physiotherapy, occupational therapy or speech therapy — it runs alongside them. Best practice is for all professions to engage in parallel, share progress and avoid fatigue or duplication. Letting the TCM practitioner see recent neurology notes and physiotherapy progress, and letting the physiotherapist know the TCM direction, produces the best overall outcome.
Four Things Families Can Do
- Medication reminders and records: daily schedule, missed-dose log, side-effect observations; bring the complete medication list to follow-ups.
- Safe environment: bathroom grab rails, non-slip mats, night lights, removed rug edges; clear space on the affected side.
- Falls prevention: 30 seconds on the bed edge before standing; rails when standing; stop if dizzy.
- Mental-health support: post-stroke depression is not uncommon. If the patient becomes withdrawn, low, unwilling to practise or sleeps poorly, discuss with the family doctor or psychiatry — do not just file it under "old age and unhappiness".
How Aspira TCM Clinic Supports Post-Stroke Rehab
Aspira's approach to post-stroke sequelae:
- Reviewing neurology discharge summary, follow-up notes and imaging reports
- Full medication-list review (especially antiplatelets, anticoagulants, antihypertensives, glucose-lowering)
- Concurrent TCM differentiation and physiotherapy functional assessment (Ms Lau On-yu holds dual qualifications as physiotherapist (PT 103352) and in TCM, allowing acupuncture to flow directly into physiotherapy within one team)
- Setting acupuncture and physiotherapy frequency that consciously avoids overlap with the neurology rehab schedule to prevent fatigue
- Teaching families home-exercise routines and safe-environment adjustments
- Planning staged review points
- Any new symptoms trigger a recommendation to return to neurology — acute issues are not handled in the clinic
FAQ | Post-Stroke Acupuncture Rehabilitation
Q1: How soon after a stroke can acupuncture start?
The general rule is that once the acute phase is over (1–2 weeks post-stroke and neurology has confirmed stability), acupuncture can be considered. Actual start timing must be jointly evaluated by neurology and the registered TCM practitioner — not decided unilaterally. Once discharged with neurology follow-up notes, you can bring the reports for an initial TCM assessment and then decide on the start date.
Q2: Will acupuncture interfere with blood thinners?
Acupuncture uses fine needles at shallow depth and generally does not affect blood-thinner efficacy. However, for patients on warfarin with INR above the therapeutic range, or those on new oral anticoagulants (DOACs) with abnormal coagulation, point location and depth need careful adjustment. Bring a complete medication list to follow-up.
Q3: Is there still a benefit after the golden window?
Yes — but progress is usually slower. Meaningful gains remain possible 6 to 12 months post-stroke; beyond 1 year is the maintenance phase, focused on preventing decline, avoiding complications and improving quality of life. Even in long-standing post-stroke patients, acupuncture and physiotherapy can still help with pain, spasticity, balance and self-care.
Q4: Can slurred speech be treated with acupuncture?
TCM management of dysarthria typically combines scalp acupuncture, sublingual points and related body points, alongside speech therapy. Outcomes vary with lesion location, severity and time of initiation. If swallowing difficulty is present (choking on water or food), assessment by a speech therapist must come first — aspiration pneumonia risk is high and TCM should not handle this alone.
Q5: Can acupuncture and physiotherapy be done on the same day?
Usually yes. A common arrangement is acupuncture first then physiotherapy (or vice versa) with a 30-minute to 1-hour break between. For frail or easily fatigued older adults, alternating days is recommended. Specific frequency and order is coordinated by the team.
Disclaimer: This article is for general health education only and does not replace individual diagnosis, investigation, medication or treatment. For any post-stroke patient, the use of acupuncture, physiotherapy or Chinese herbal medicine must be jointly assessed by neurology, registered TCM practitioner and physiotherapist; any medication change must be discussed with the treating doctor first.
Disclaimer: This article is for health education and reference purposes only and does not constitute medical advice, diagnosis, or treatment. Each patient's condition is unique and treatment outcomes vary. Please consult a registered TCM practitioner or qualified healthcare professional for health concerns.
Want to learn more? WhatsApp us for a free consultation
Book via WhatsAppExplore our full range of treatments: Traditional TCM Services
Related Articles

Do Oysters, Maca and Deer Antler Boost Male Vitality? 5 Myths
Do aphrodisiac foods actually work? This article opens with a rating table (effective / partly effective / effective within a TCM framework / weak evidence / no strong evidence), reviews the Chinese and Western medical evidence behind oysters, maca, deer antler, sea cucumber and Chinese chives, distils the 3 shared traits of foods that genuinely support male sexual function, and flags 3 commonly eaten items that can actually harm performance.

Male Menopause Through the TCM Lens: 5 Signs in Men Over 40
Unexplained fatigue, irritability, lower libido, poorer sleep and a growing belly after 40 are not just ageing or work stress — they may be male menopause. This article begins with a five-sign self-check, sets out three TCM patterns (kidney-yang deficiency, kidney-yin deficiency, liver-and-kidney insufficiency) with matching improvements, and compares the two treatment routes — testosterone replacement therapy versus TCM constitutional care.
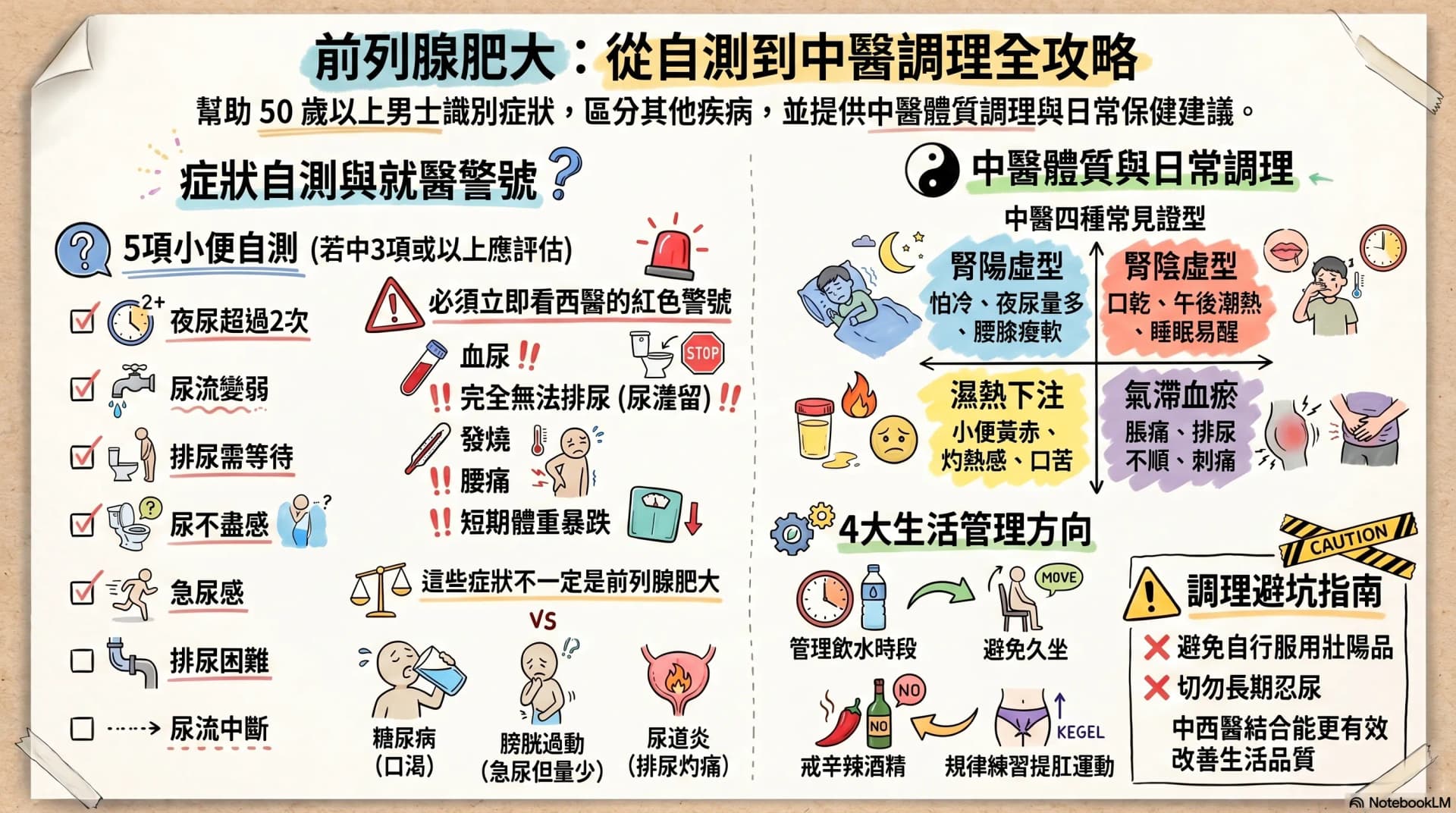
Enlarged Prostate: Are Nocturia and a Weak Stream Warning Signs?
After age 50, urinary frequency, nocturia, a weaker stream and having to urinate in stages may not simply be ageing. This article opens with a 7-symptom self-check, then sets out warning signs that warrant seeing a Western doctor immediately, four TCM constitution patterns, and four daily care directions any man can start with — helping you or your father decide the next step.