Endometriosis: Causes and TCM Care for Painful Periods, Infertility and Dyspareunia
Endometriosis is one of the most under-recognised chronic conditions in women's health, possible from menarche through to menopause. This article covers common symptoms, lesion locations, five TCM pattern directions, the different TCM approaches during and outside menstruation, how care coordinates with fertility planning, and warning signs that should not be left to TCM alone.
Medical review: Dr. To Ching, Jenny,Registered Chinese Medicine Practitioner #009330
1-Minute Quick Answer
Endometriosis is a chronic gynaecological condition often mistaken for ordinary period pain, affecting about one in ten women of reproductive age and causing worsening cramps, dyspareunia and infertility. TCM works on blood stasis by pattern, phased across the cycle, alongside gynaecological follow-up. Sudden severe pain or a year of failed conception needs medical review first.
Endometriosis: Causes and TCM Care for Painful Periods, Infertility and Dyspareunia
 For quick reference, this image was generated by NotebookLM. Some Chinese characters may not render perfectly; we appreciate your understanding.
For quick reference, this image was generated by NotebookLM. Some Chinese characters may not render perfectly; we appreciate your understanding.
Medical review: Dr To (CMCHK 009330 | Gynaecology, TCM aesthetics, postpartum belly binding, paediatrics)
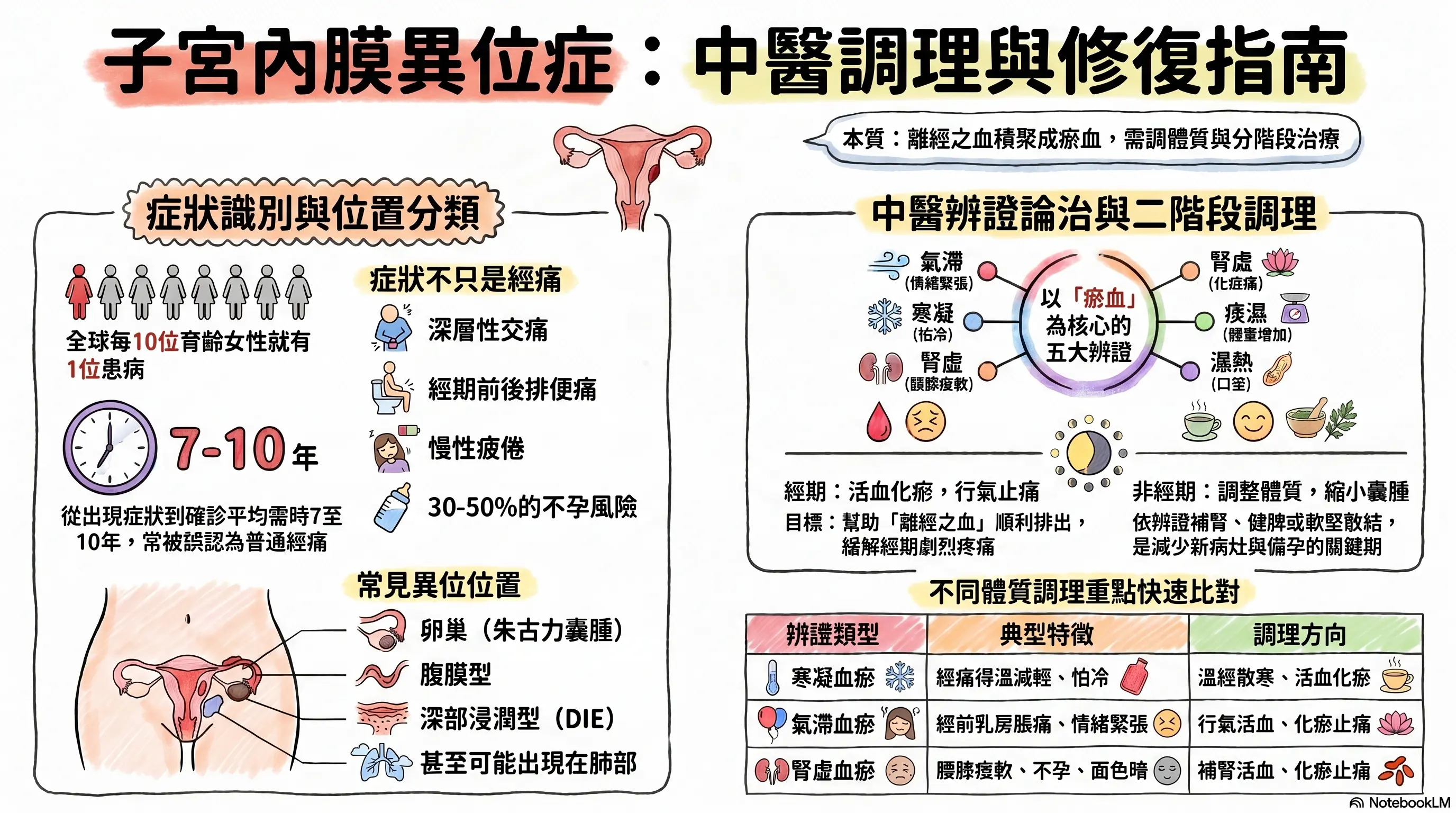
Endometriosis is one of the most under-recognised chronic conditions in women's health, and one of the most easily mis-labelled as simply "period pain". International data put the prevalence at around one in ten women of reproductive age, with onset possible from menarche through to menopause. It is directly linked to period pain, infertility, chronic pelvic pain, deep dyspareunia, bowel and bladder symptoms and, often, considerable psychological strain.
Worth noting: the global average from first symptoms to diagnosis is seven to ten years — meaning many women live with worsening pain for years without knowing what is happening, with real consequences for quality of life and fertility plans.
This article walks through common symptoms, lesion locations, the five TCM pattern directions, and the different TCM approaches taken during and outside menstruation.
1. Common Symptoms of Endometriosis
Endometriosis does not show up as "just period pain". The most common features cluster as follows:
| Domain | Common features |
|---|---|
| Menstruation | Progressive dysmenorrhoea (each month often worse; declining response to painkillers), heavier flow, longer periods, brown spotting before or after |
| Non-menstrual pelvic | Chronic lower-abdominal aching, deep pelvic heaviness, lumbosacral soreness |
| Sexual | Deep dyspareunia (especially in the days before the period), bleeding or pain that lingers after intercourse |
| Bowel | Painful defecation around menses, alternating constipation and diarrhoea, rectal bleeding in severe deep-infiltrating cases |
| Bladder | Painful urination around menses, frequency, haematuria in severe cases |
| Reproductive | Infertility (in 30–50% of patients), higher miscarriage risk |
| Systemic | Chronic fatigue, low-grade heat sensation around the period, depressive symptoms |
Worth noting: symptom severity does not always match lesion size. Small lesions can cause severe pain and larger cysts can be almost asymptomatic. If painkillers no longer control the cramps, or pain disrupts work and daily life, raise it with a gynaecologist.
2. Where Endometriotic Lesions Sit
In a normal cycle, endometrial tissue should only line the uterine cavity. In endometriosis, similar tissue appears outside the uterus, bleeding and inflaming in step with the cycle. By location and depth, the main categories are:
| Type | Common location | Notes |
|---|---|---|
| Peritoneal | Pelvic peritoneal surface, pouch of Douglas | Small, superficial lesions; often only seen at laparoscopy |
| Ovarian (endometrioma, "chocolate cyst") | Within the ovary | Cysts containing old blood (chocolate-coloured fluid); visible on ultrasound |
| Deep infiltrating endometriosis (DIE) | Pouch of Douglas, uterosacral ligaments, bowel wall, bladder, ureter | Infiltrating more than 5 mm; often linked to severe pain, dyspareunia, bowel or urinary symptoms |
| Adenomyosis | Within the myometrium | Strictly a separate entity but often co-exists; presents with severe dysmenorrhoea, heavy flow and an enlarged uterus |
| Rare sites | Diaphragm, pleura, lung, Caesarean or perineal scar | Symptoms depend on site (e.g. catamenial pneumothorax, cyclical scar pain) |
Laparoscopy with histology remains the diagnostic gold standard. Pelvic ultrasound is sensitive for ovarian cysts; deep-infiltrating disease may need MRI. CA-125 has limited sensitivity and specificity and cannot stand alone.
3. The TCM View: Five Pattern Directions
The core TCM idea is that this condition reflects blood out of its proper channel, accumulating in the pelvis as stasis. Why the stasis arises differs from patient to patient. The five most common patterns:
| Pattern | Common features | Direction |
|---|---|---|
| Qi-blood stagnation | Premenstrual tension, breast tenderness, dark menstrual blood with clots | Move qi, move blood, relieve pain |
| Cold-stasis | Pain eased by warmth, cold extremities, preference for warm drinks, pale tongue with white coating | Warm the channels, dispel cold, move blood |
| Kidney-deficient stasis | Lower-back soreness, late menarche, light periods, infertility, dull complexion | Tonify the kidney and move blood |
| Phlegm-stasis | Fuller body type, increased discharge, prominent cysts, greasy tongue coating | Resolve phlegm-damp, soften masses, move blood |
| Damp-heat stasis | Premenstrual heat sensation, vulvar itching, yellow urine, yellow greasy tongue coating | Clear heat, drain damp, move blood |
Patterns often overlap (for example, "cold-stasis with kidney deficiency" or "qi-blood stagnation with phlegm-damp"). Prescriptions are decided by a registered TCM practitioner from tongue, pulse, menstrual history and imaging.
In plainer language: "blood stasis" describes poorly circulating, accumulated blood; "blood out of its channel" is blood that has not flowed where it should. The idea sits close to the modern description of retrograde menstruation and impaired clearance of menstrual tissue.
4. TCM Care: Different Approaches Inside and Outside Menstruation
A distinctive feature of TCM endometriosis care is that the menstrual and post-menstrual phases use different directions:
During menstruation (from onset to end of period):
- Direction: move blood, regulate qi, relieve pain
- Goal: help "blood out of its channel" flow more cleanly and reduce pain
- External therapies often used: warming patches, moxibustion, acupuncture at Guanyuan, Sanyinjiao, Shiqizhuixia
Between periods (after the period ends until the next):
- Direction: by pattern — tonifying the kidney, supporting the spleen, resolving phlegm, softening masses, clearing heat
- Goal: reduce cyst size, slow new lesion formation, improve constitution
- This is the "foundation" phase; long-term outcomes mainly rest on the care given here
Pace: one observation cycle is three menstrual cycles. Mild-to-moderate patients often see pain easing and the cycle settling within three to six months; ovarian cysts need parallel ultrasound monitoring.
5. Working Alongside Fertility Care
About 30–50% of endometriosis patients experience infertility. TCM's role across the fertility journey:
| Phase | TCM role |
|---|---|
| Trying naturally | Cycle-based therapy, ovulation support, pain relief |
| Before IUI / IVF | Nourish yin and blood pre-retrieval; move blood to improve pelvic environment |
| Around transfer | Tonify qi and blood, support the kidney for pregnancy maintenance, reduce medication side effects |
| Around surgery | Move blood pre-op for clearer surgical field; speed recovery and reduce recurrence post-op |
Coordination is best worked out with the gynaecologist or fertility specialist.
6. Warning Signs — When TCM Alone Is Not Enough
These should not be treated as simply "period pain":
- Sudden severe abdominal pain with vomiting and fever (suspected cyst rupture or torsion — emergency)
- Heavy bleeding outside the period; worsening anaemia
- Blood in stool or urine (possible deep-infiltrating involvement of bowel or bladder)
- Acute lower-abdominal pain with low blood pressure or fainting
- Trying to conceive for over 12 months (or 6 months if over 35) without success
- A new palpable pelvic mass
TCM does not replace imaging, laparoscopic surgery or hormonal therapy. Ovarian cysts need regular ultrasound monitoring with the gynaecologist; surgery is sometimes needed.
7. How Aspira TCM Clinic Assesses
Before the first visit, please bring:
- A menstrual log over the past six months (with pain score, flow, symptoms)
- Recent gynaecological reports (ultrasound, MRI, CA-125)
- Any surgical and pathology reports (if laparoscopy has been done)
- A current medication list (NSAIDs, COCP, progestins, GnRH agents)
- Any pregnancy plans
Dr To designs the programme around pattern, cycle phase and fertility goals, and discusses how it dovetails with Western treatment.
— Dr To | Registered Chinese Medicine Practitioner (Gynaecology, TCM Aesthetics, Postpartum Belly Binding, Paediatrics) Reg. No.: 009330 Aspira TCM Clinic
Frequently Asked Questions
Q1: I am already on painkillers for cramps — can I take Chinese herbs at the same time?
Yes. The herbal direction is chosen to complement the medications: during menstruation, movement of blood and pain relief (not at odds with NSAIDs); between periods, constitutional work. As the constitution improves, some patients can taper painkiller use under the gynaecologist's guidance. Decisions about stopping painkillers rest with the doctor.
Q2: Can acupuncture improve endometriosis?
It can play a supportive role. Acupuncture has clinical support for managing "blood out of its channel" and stasis, with points such as Guanyuan, Qihai, Sanyinjiao, Shiqizhuixia and Taichong commonly used. It can help with:
- Reducing dysmenorrhoea and deep pelvic ache
- Improving cycle stability
- Working alongside cycle-based herbal therapy for better overall outcomes
- Supporting the pelvic environment around IVF retrieval and transfer
Important to note: acupuncture cannot "eliminate" endometriotic lesions, nor does it replace imaging follow-up and surgery. With large ovarian cysts, the position and depth of abdominal needling must be judged carefully by a registered practitioner, and direct needling over the cyst site is avoided.
Q3: I've already had laparoscopic excision — do I still need TCM?
It is worth considering. Recurrence within one year of surgery is around 10–20%, and up to 50% within five years. The three to six months after surgery is an important TCM window. Working on stasis, kidney support and cycle regulation can lower recurrence, while also helping recovery and overall constitution.
Q4: While on GnRH therapy, my periods have stopped — is there still a role for TCM?
Yes. The TCM role during GnRH treatment is to manage the "pseudo-menopausal" side effects — hot flushes, bone-density concerns, mood swings, vaginal dryness — typically working on kidney-yin, liver and blood. The transition after stopping GnRH is also an important window for restoring cycle regularity.
Q5: Can TCM dissolve an ovarian "chocolate cyst"?
For small cysts (under 3–4 cm), long-term pattern-based TCM care has been associated clinically with size reduction in some patients; shrinkage cannot be guaranteed in every case. Larger cysts (over 5 cm) or rapidly growing cysts still need surgical management as the main approach, with TCM supporting pre- and post-operative care.
Living with Endometriosis? Book a Consultation
If you have a diagnosis of endometriosis or have been struggling with severe dysmenorrhoea, dyspareunia or infertility, please bring your gynaecological reports, menstrual log and current medication list before booking a consultation with Dr To. Any decision about painkillers, hormonal therapy or surgery must rest with your gynaecologist. For sudden severe pain with vomiting and fever, please attend the emergency department.
How to book:
- WhatsApp: Book here
- Phone: 2110 9337
- Address: Unit 2706, 27/F, Saxon Tower, 7 Cheung Shun Street, Lai Chi Kok
Disclaimer: This article is for general health education only and does not replace individual diagnosis, examination, medication or treatment advice. Endometriosis is a chronic gynaecological condition; treatment must be individualised and developed jointly between a gynaecologist and a registered TCM practitioner. Decisions about painkillers, hormonal therapy or surgery should first be discussed with the prescribing doctor.
Disclaimer: This article is for health education and reference purposes only and does not constitute medical advice, diagnosis, or treatment. Each patient's condition is unique and treatment outcomes vary. Please consult a registered TCM practitioner or qualified healthcare professional for health concerns.
Further Reading
Hand-picked related articles and real cases to read next.
A Self-Check Guide to 4 Types of Menstrual Pain and Relief Tips
Menstrual pain is not something you simply have to endure. This guide explains the difference between primary and secondary dysmenorrhea, outlines four common TCM patterns, highlights five warning signs that need medical review, and offers practical relief strategies for everyday care.
Polycystic Ovary Syndrome (PCOS): Causes and TCM Care for Menstrual Irregularity, Hair Growth, Acne and Infertility
PCOS is not simply "irregular periods" — it is a long-term condition spanning the endocrine, metabolic and reproductive axes. This article covers common symptoms, four TCM pattern directions (kidney deficiency, phlegm-damp, liver stagnation, qi-blood stagnation), TCM care (cycle-based therapy, acupuncture, weight and insulin resistance management), how to coordinate with Western treatment, and the investigations and warning signs to know.
Want to learn more? WhatsApp us for a free consultation
Book via WhatsAppExplore our full range of treatments: Traditional TCM Services
Related Articles

Do Oysters, Maca and Deer Antler Boost Male Vitality? 5 Myths
Do aphrodisiac foods actually work? This article opens with a rating table (effective / partly effective / effective within a TCM framework / weak evidence / no strong evidence), reviews the Chinese and Western medical evidence behind oysters, maca, deer antler, sea cucumber and Chinese chives, distils the 3 shared traits of foods that genuinely support male sexual function, and flags 3 commonly eaten items that can actually harm performance.

Male Menopause Through the TCM Lens: 5 Signs in Men Over 40
Unexplained fatigue, irritability, lower libido, poorer sleep and a growing belly after 40 are not just ageing or work stress — they may be male menopause. This article begins with a five-sign self-check, sets out three TCM patterns (kidney-yang deficiency, kidney-yin deficiency, liver-and-kidney insufficiency) with matching improvements, and compares the two treatment routes — testosterone replacement therapy versus TCM constitutional care.
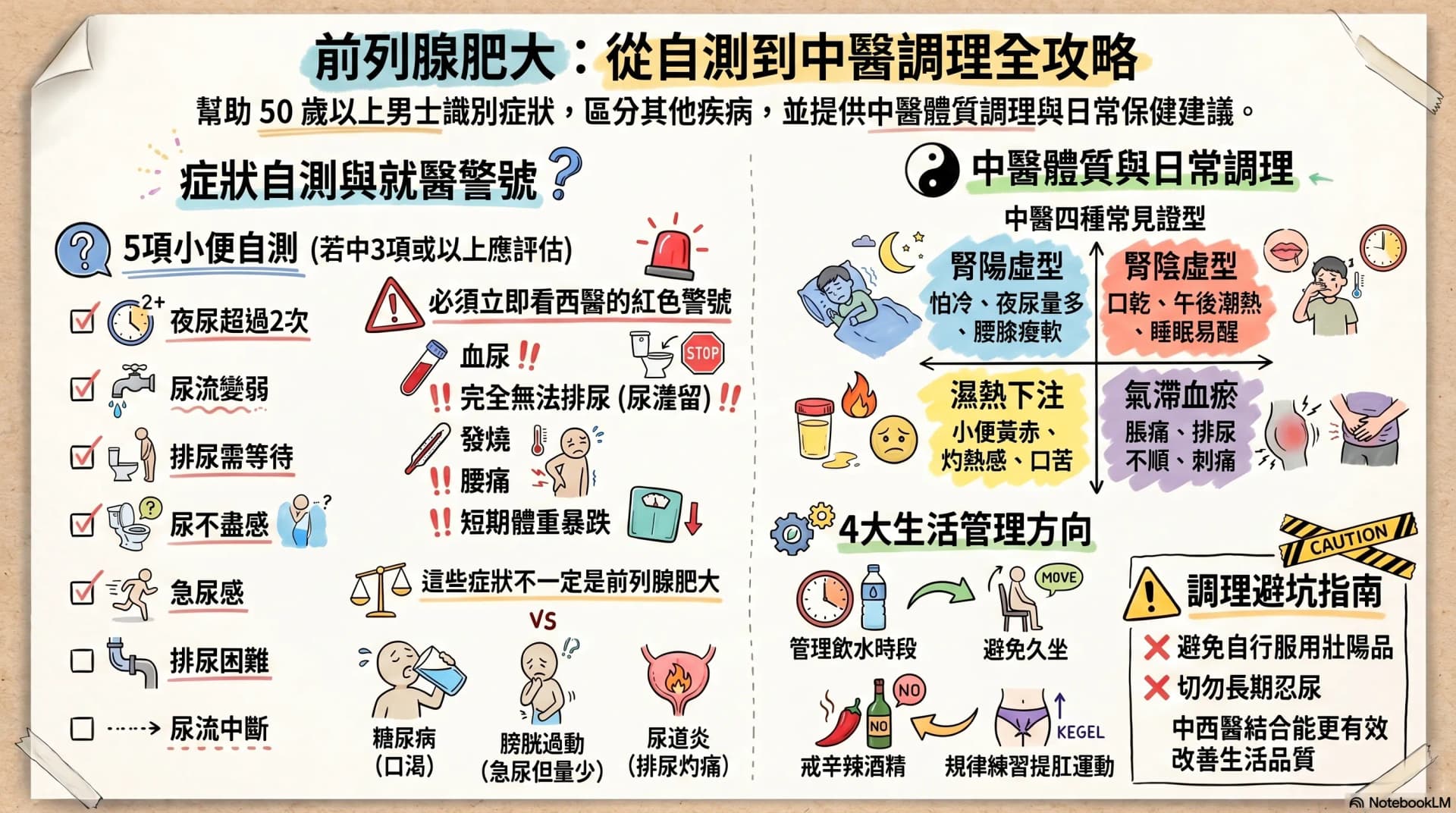
Enlarged Prostate: Are Nocturia and a Weak Stream Warning Signs?
After age 50, urinary frequency, nocturia, a weaker stream and having to urinate in stages may not simply be ageing. This article opens with a 7-symptom self-check, then sets out warning signs that warrant seeing a Western doctor immediately, four TCM constitution patterns, and four daily care directions any man can start with — helping you or your father decide the next step.