PCOS Renamed PMOS — Symptom Self-Check and Combined Western–TCM Care
PCOS has been renamed PMOS (Polyendocrine Metabolic Ovarian Syndrome) to emphasise that it is not only a gynaecological condition but a metabolic one. This article walks through how PMOS develops (Western and TCM views), a three-category nine-point symptom self-check, the combined Western–TCM treatment plan, and practical low-GI diet and resistance-training steps every patient can start at home.
Medical review: Dr. Chan Wing Kiu, Joanne,Registered Chinese Medicine Practitioner #009463
1-Minute Quick Answer
Following the 2026 Lancet expert consensus, PCOS has been renamed PMOS, emphasising that it is not only a gynaecological condition but a long-term endocrine and metabolic disorder; diagnosis rests on the metabolic picture, not ultrasound alone. This guide offers a nine-point self-check across three categories; meeting three or more warrants a gynaecological or endocrine workup first.
PCOS Renamed PMOS — Symptom Self-Check and Combined Western–TCM Care
 For quick reference, this image was generated by NotebookLM. Some Chinese characters may not render perfectly; we appreciate your understanding.
For quick reference, this image was generated by NotebookLM. Some Chinese characters may not render perfectly; we appreciate your understanding.
Medical review: Dr Chan (CMCHK 009463 | Geriatric gynaecology, perimenopause, uterine fibroids, internal medicine)
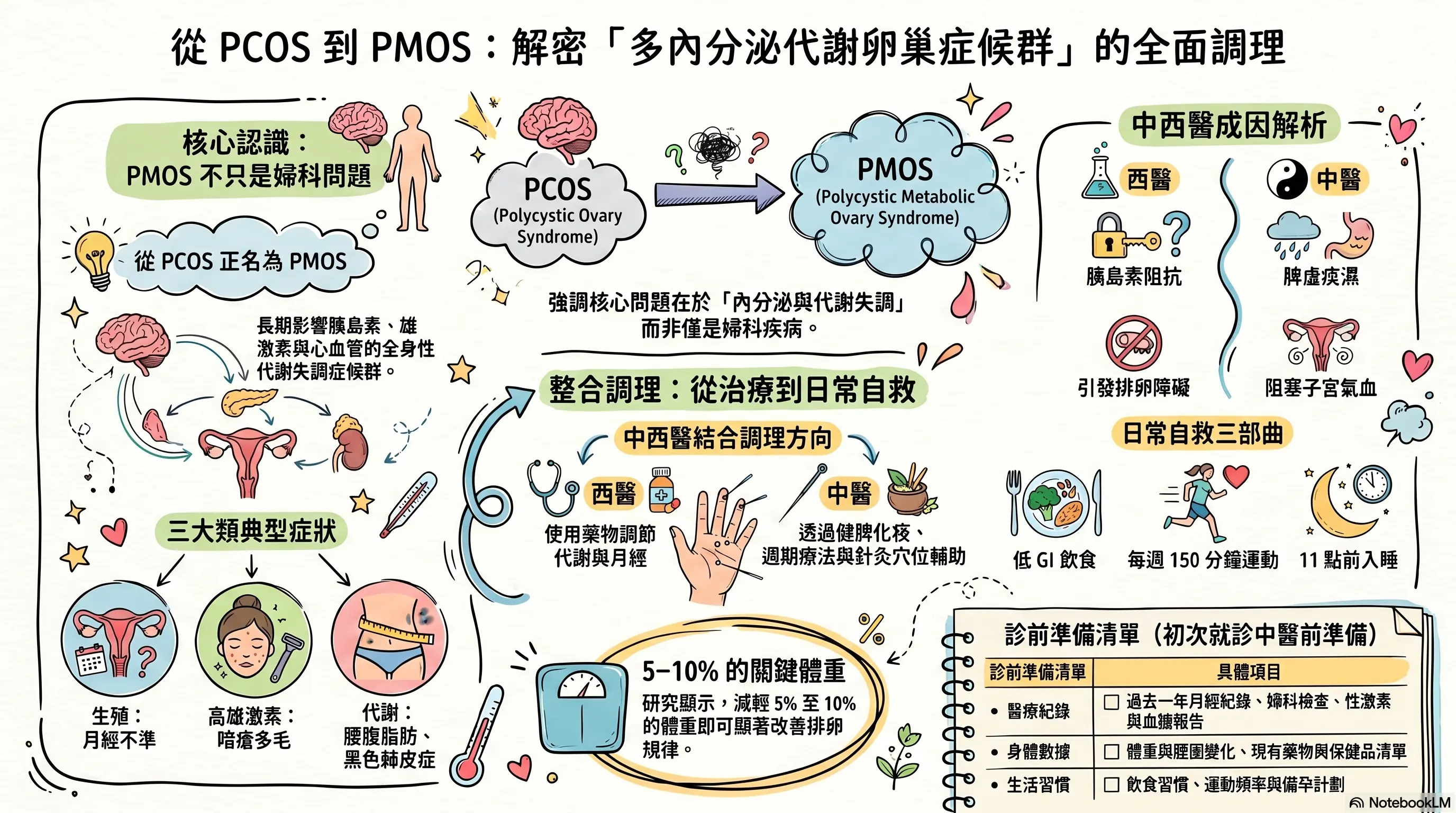
When women first hear the diagnosis Polycystic Ovary Syndrome (PCOS), the picture in their head is usually small cysts on the ovary, irregular periods and possible fertility difficulties. A 2026 expert consensus published in The Lancet¹ has, however, formally renamed the condition PMOS — Polyendocrine Metabolic Ovarian Syndrome. The new name draws attention to a word that used to be easily missed: Metabolic.
In other words, PMOS is not only a gynaecological condition. It is a long-term endocrine and metabolic disorder whose reach extends far beyond the ovaries and the menstrual cycle — to insulin, androgens, body weight, skin, mood, and long-term cardiovascular risk. This also explains why many patients do not show the classical "string of pearls" on ultrasound yet still struggle with irregular cycles, acne, hair growth, abdominal weight gain and stalled weight loss — diagnosis was never meant to hinge on a single ultrasound image.
This article opens with a three-category nine-point symptom self-check, then walks through the Western and TCM accounts of how PMOS develops, and how the two systems coordinate.
1. PMOS Symptom Self-Check: Three Categories, Nine Items
The nine items below fall into three categories. If you meet three or more, please arrange a gynaecological or endocrine workup and consider TCM care alongside.
1. Reproductive and menstrual symptoms (ovarian dysfunction)
- Oligo-ovulation or amenorrhoea: cycles drift longer (over 35–45 days), sometimes only once every six to twelve months
- Volume and quality changes: lighter periods, dark or blackish flow, large clots
- Fertility difficulty: irregular ovulation makes natural conception harder; some need assisted reproduction
2. Hyperandrogenic symptoms (more masculine appearance)
- Hirsutism: hair appears in atypical female sites — upper lip, chin, chest, midline below the umbilicus, inner thighs
- Persistent acne: well after the teenage years, the jawline, chin and back continue to produce large painful cystic lesions; very oily skin
- Male-pattern hair loss: a widening parting at the crown, thinner hair, noticeable loss — the hairline itself usually does not recede
3. Endocrine and metabolic symptoms (the heart of the PMOS rename)
- Central (apple-shaped) obesity: limbs may not be heavy, but fat collects around the waist and is very hard to lose — many patients describe "putting on weight from water"
- Acanthosis nigricans: persistent dark, thickened, velvety patches at the back of the neck, underarms, groin and inner thighs
- Reactive hypoglycaemia, mood and sleep swings: strong sugar cravings shortly after meals; tremor, palpitations, cold sweats; over time, anxiety, depression, binge eating and sleep-disordered breathing (loud snoring at night)
Worth noting: not every PMOS patient shows ovarian cysts on ultrasound. Many lean patients look outwardly unaffected but their blood work and symptom profile already meet several criteria — this is precisely what the PMOS rename emphasises: diagnosis rests on the metabolic and endocrine picture as a whole, not on a single imaging study.
2. How PMOS Develops — the Western and TCM Views
The Western view: insulin resistance to ovarian disruption
Modern life — refined food, high sugar, low activity, high stress, short sleep — pushes a single core problem over time: insulin resistance (cells respond poorly to insulin, blood sugar cannot enter cells to be used).
Insulin resistance sets off a chain:
- The pancreas secretes more insulin to hold blood sugar steady (hyperinsulinaemia)
- High insulin directly drives the ovary to secrete excess androgens (testosterone)
- Excess androgens stall follicle maturation — follicles are stuck "half-mature" and cannot ovulate
- Multiple half-mature follicles line the ovarian surface — the classical "string of pearls" image
Excess androgens drive acne, hair growth and male-pattern hair loss; insulin resistance drives abdominal fat accumulation, post-meal fatigue, sugar cravings, and long-term cardiovascular and diabetic risk. PMOS is therefore not "a problem in one organ" — it is a whole-body metabolic imbalance that shows up in the ovary.
The TCM view: spleen-deficient phlegm-damp, channels obstructed
The TCM understanding centres on "spleen deficiency with phlegm-damp". The spleen-stomach is responsible for transforming food and fluid into qi and blood. When the spleen runs low, what should become qi and blood instead lingers as phlegm-damp — excess metabolic by-product and fluid the body cannot clear.
Over time, phlegm-damp settles around the abdomen, uterus and ovaries, obstructing the channels and impairing the flow of qi and blood to the reproductive organs. The result is the familiar picture: scanty periods, amenorrhoea and difficulty conceiving. In clinic, PMOS patients often present with "spleen-deficient phlegm-damp" overlaid with kidney deficiency or liver-qi stagnation, requiring a registered TCM practitioner to differentiate from tongue, pulse and the overall picture.
In simpler terms: "phlegm-damp" describes built-up metabolic by-products and fluid; "spleen deficiency" describes a digestion-and-metabolism baseline that is running low.
3. Combined Western–TCM Care
Western strategy: symptom control and long-term protection
By goal, the common tools are:
| Goal | Common approach |
|---|---|
| Improve insulin resistance | Metformin; inositol supplementation |
| Regulate cycles, control androgens | Combined oral contraceptive pill, anti-androgens |
| Protect the endometrium (long amenorrhoea) | Cyclical progestins |
| Induce ovulation (fertility) | Letrozole, clomiphene |
| Weight management | Dietary counselling; weight-loss medication where indicated |
| Hirsutism, acne | Dermatology referral |
Choices and dosing are set by a gynaecologist or endocrinologist with regular review of side effects and long-term outcomes.
TCM strategy: tonify the spleen, resolve phlegm, support the kidney, move blood
TCM in PMOS is not simply "bringing the period back". The aim is to clear phlegm-damp and restart the spleen-stomach and ovarian rhythm. Common directions:
- Tonify the spleen, resolve phlegm — addressing the core mechanism, with spleen-strengthening and damp-resolving herbs
- Tonify the kidney, move blood — building the reproductive-endocrine baseline and reopening channels obstructed by phlegm-stasis
- Cycle-based therapy — different directions in the post-menstrual, ovulatory, premenstrual and menstrual phases
- Acupuncture — points such as Guanyuan, Qihai, Sanyinjiao, Zusanli, Fenglong, Taichong
One observation cycle is generally three menstrual cycles, aiming for steadier cycles and progressively more regular ovulation.
Daily self-help: three things you can start today
Medical care is only half of it. Lifestyle change is decisive in the long-term stability of PMOS. Three places to begin:
- A strict low-GI diet. Cut refined carbohydrates (white rice, white bread, refined sweets, sugary drinks); switch to brown rice, oats, whole grains, adequate protein and fibre — so blood sugar stops spiking and crashing
- At least 150 minutes per week of moderate cardio plus resistance training. Muscle is the body's best blood-sugar furnace; building muscle and reducing fat improves insulin sensitivity. Even without weight loss, "swapping the composition" is meaningful
- Sleep and stress management. Sleep before 11 pm with seven or more hours; chronic stress and short sleep worsen insulin resistance and androgen balance
Research shows a 5–10% weight reduction is often enough to noticeably restore ovulation. For many PMOS patients, dietary and movement changes outperform any single medication or formula on their own.
4. How Aspira TCM Clinic Assesses PMOS
Before the first visit, please bring:
- A menstrual log over the past year (dates, flow, symptoms)
- Recent gynaecological reports (ultrasound, reproductive hormones, AMH, fasting insulin, HbA1c)
- Weight and waist changes over time
- A current medication and supplement list (COCP, metformin, inositol)
- An outline of diet and exercise habits
- Any pregnancy plans
Dr Chan tailors the programme to pattern, cycle phase and fertility goals, and:
- Keeps the gynaecologist or endocrinologist informed (written notes on the herbal direction, passed via the patient)
- Will not advise stopping Western medication on the patient's own
- Provides concrete low-GI dietary, exercise and sleep recommendations alongside
— Dr Chan Wing Kiu | Registered Chinese Medicine Practitioner (Geriatric Gynaecology, Internal Medicine) Reg. No.: 009463 Aspira TCM Clinic
Frequently Asked Questions
Q1: Can someone of normal weight still have PMOS?
Yes. Around 20–30% of PMOS patients have "lean PMOS" — BMI within the normal range, yet still with insulin resistance, raised androgens and irregular cycles. Care for this group focuses on blood-sugar stability rather than weight loss, with TCM emphasising the kidney, liver and blood movement.
Q2: Does PMOS always require lifelong medication?
Not necessarily. Whether medication is needed, and for how long, depends on symptoms, goals (cycle control, fertility, endometrial protection) and how far lifestyle change has progressed. Many patients, with strict low-GI eating, regular movement and TCM care, gradually reduce medication under the gynaecologist's guidance. Any decision to stop medication rests with the prescribing doctor and should not be self-decided.
Q3: Is TCM appropriate during fertility planning?
Yes — fertility is one of TCM's strong suits in PMOS care. The role is to restore ovulatory rhythm, regulate the cycle, and coordinate with ovulation tracking or induction medications. Starting three to six months before active attempts at conception is a reasonable plan.
Q4: Can acanthosis nigricans, acne or hirsutism be addressed by TCM alone?
Partly, but not entirely. Acanthosis nigricans reflects insulin resistance — the core treatment lies in improving insulin sensitivity (diet, movement, medication where indicated); the pigmentation tends to fade as metabolism settles. Acne and hirsutism take time (hirsutism usually six months or more); clearing liver-stomach heat and resolving phlegm-damp via TCM has clinical support alongside.
Q5: Do Chinese herbs interact with the contraceptive pill or metformin?
Co-prescribing is generally safe, but the TCM practitioner needs to know exactly which pill and dose, so the herbal direction does not interfere. Metformin's gastrointestinal side effects can be eased by spleen-stomach support. Disclose every medication you are on — that is the foundation of safe coordination.
Diagnosed with PMOS or Recognising the Symptoms? Book a Consultation
If you meet three or more of the symptoms above, or already have a PCOS / PMOS diagnosis and would like TCM to support metabolic and cycle care, please bring your gynaecological reports, menstrual log, weight history and current medication list before booking a consultation with Dr Chan. Any change to the contraceptive pill, metformin or ovulation-induction medication should first be discussed with the prescribing doctor.
How to book:
- WhatsApp: Book here
- Phone: 2110 9337
- Address: Unit 2706, 27/F, Saxon Tower, 7 Cheung Shun Street, Lai Chi Kok
Disclaimer: This article is for general health education only and does not replace individual diagnosis, examination, medication or treatment advice. PMOS is a long-term endocrine and metabolic condition; treatment plans must be individualised and built jointly by a gynaecologist or endocrinologist and a registered TCM practitioner. Any change to oral contraceptives, metformin or ovulation-induction medications must first be discussed with the prescribing doctor.
References
- The Lancet (2026) — Expert consensus on renaming PCOS to PMOS (Polyendocrine Metabolic Ovarian Syndrome). https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(26)00717-8/fulltext
Disclaimer: This article is for health education and reference purposes only and does not constitute medical advice, diagnosis, or treatment. Each patient's condition is unique and treatment outcomes vary. Please consult a registered TCM practitioner or qualified healthcare professional for health concerns.
Further Reading
Hand-picked related articles and real cases to read next.
Polycystic Ovary Syndrome (PCOS): Causes and TCM Care for Menstrual Irregularity, Hair Growth, Acne and Infertility
PCOS is not simply "irregular periods" — it is a long-term condition spanning the endocrine, metabolic and reproductive axes. This article covers common symptoms, four TCM pattern directions (kidney deficiency, phlegm-damp, liver stagnation, qi-blood stagnation), TCM care (cycle-based therapy, acupuncture, weight and insulin resistance management), how to coordinate with Western treatment, and the investigations and warning signs to know.
A Self-Check Guide to 4 Types of Menstrual Pain and Relief Tips
Menstrual pain is not something you simply have to endure. This guide explains the difference between primary and secondary dysmenorrhea, outlines four common TCM patterns, highlights five warning signs that need medical review, and offers practical relief strategies for everyday care.
How TCM Reads Vaginal Discharge — Fishy, Yellow-Green, Bloody and Heavy
Persistent changes in vaginal discharge are health signals worth attending to. This article uses four dimensions — colour, smell, texture and volume — to help you tell normal from abnormal, outlines six common abnormal presentations, four TCM pattern directions, and how TCM works on the root constitution to reduce recurrence rather than only relieving itch or treating an infection.
Want to learn more? WhatsApp us for a free consultation
Book via WhatsAppExplore our full range of treatments: Traditional TCM Services
Related Articles

Do Oysters, Maca and Deer Antler Boost Male Vitality? 5 Myths
Do aphrodisiac foods actually work? This article opens with a rating table (effective / partly effective / effective within a TCM framework / weak evidence / no strong evidence), reviews the Chinese and Western medical evidence behind oysters, maca, deer antler, sea cucumber and Chinese chives, distils the 3 shared traits of foods that genuinely support male sexual function, and flags 3 commonly eaten items that can actually harm performance.

Male Menopause Through the TCM Lens: 5 Signs in Men Over 40
Unexplained fatigue, irritability, lower libido, poorer sleep and a growing belly after 40 are not just ageing or work stress — they may be male menopause. This article begins with a five-sign self-check, sets out three TCM patterns (kidney-yang deficiency, kidney-yin deficiency, liver-and-kidney insufficiency) with matching improvements, and compares the two treatment routes — testosterone replacement therapy versus TCM constitutional care.
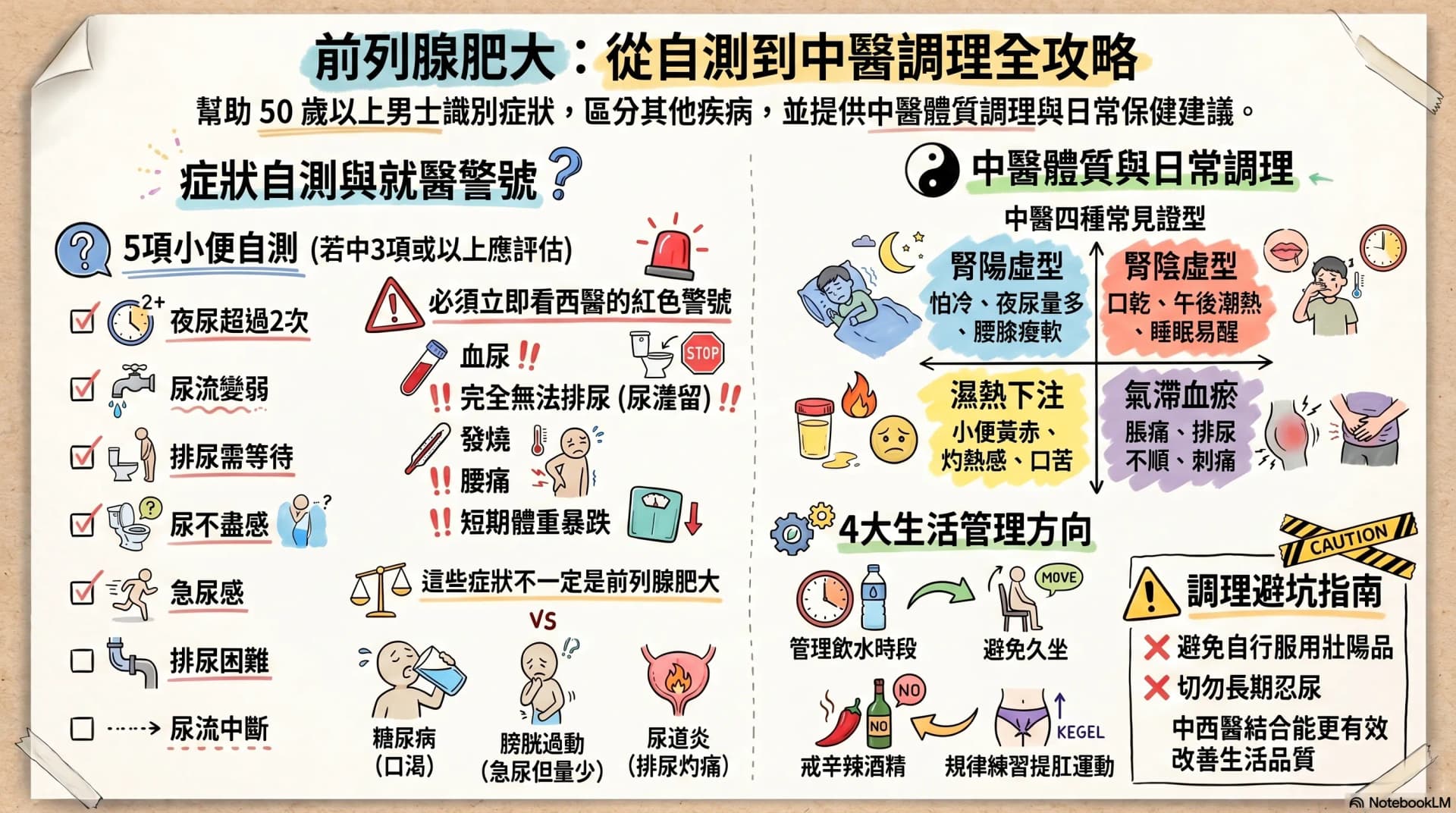
Enlarged Prostate: Are Nocturia and a Weak Stream Warning Signs?
After age 50, urinary frequency, nocturia, a weaker stream and having to urinate in stages may not simply be ageing. This article opens with a 7-symptom self-check, then sets out warning signs that warrant seeing a Western doctor immediately, four TCM constitution patterns, and four daily care directions any man can start with — helping you or your father decide the next step.