ADHD in Children: Symptoms and the TCM Approach
ADHD is a neurodevelopmental condition, not a parenting issue, and diagnosis must come from a developmental paediatrician or child psychiatrist. This article walks through the three ADHD presentations and their symptoms, the workup involved, four TCM pattern directions, how TCM can complement (not replace) mainstream treatment, five things parents can start today, and the warning signs that require Western medical attention first.
Medical review: Dr. To Ching, Jenny,Registered Chinese Medicine Practitioner #009330
1-Minute Quick Answer
ADHD is a neurodevelopmental condition, not a parenting issue, and must be diagnosed by a developmental paediatrician or child psychiatrist. TCM plays only a supportive role, working by pattern on sleep, mood and digestion so mainstream care lands better; it does not replace behavioural therapy or medication. Without a formal diagnosis, see a paediatrician first.
ADHD in Children: Symptoms and the TCM Approach
 For quick reference, this image was generated by NotebookLM. Some Chinese characters may not render perfectly; we appreciate your understanding.
For quick reference, this image was generated by NotebookLM. Some Chinese characters may not render perfectly; we appreciate your understanding.
Medical review: Dr To (CMCHK 009330 | Gynaecology, TCM aesthetics, postpartum belly binding, paediatrics)
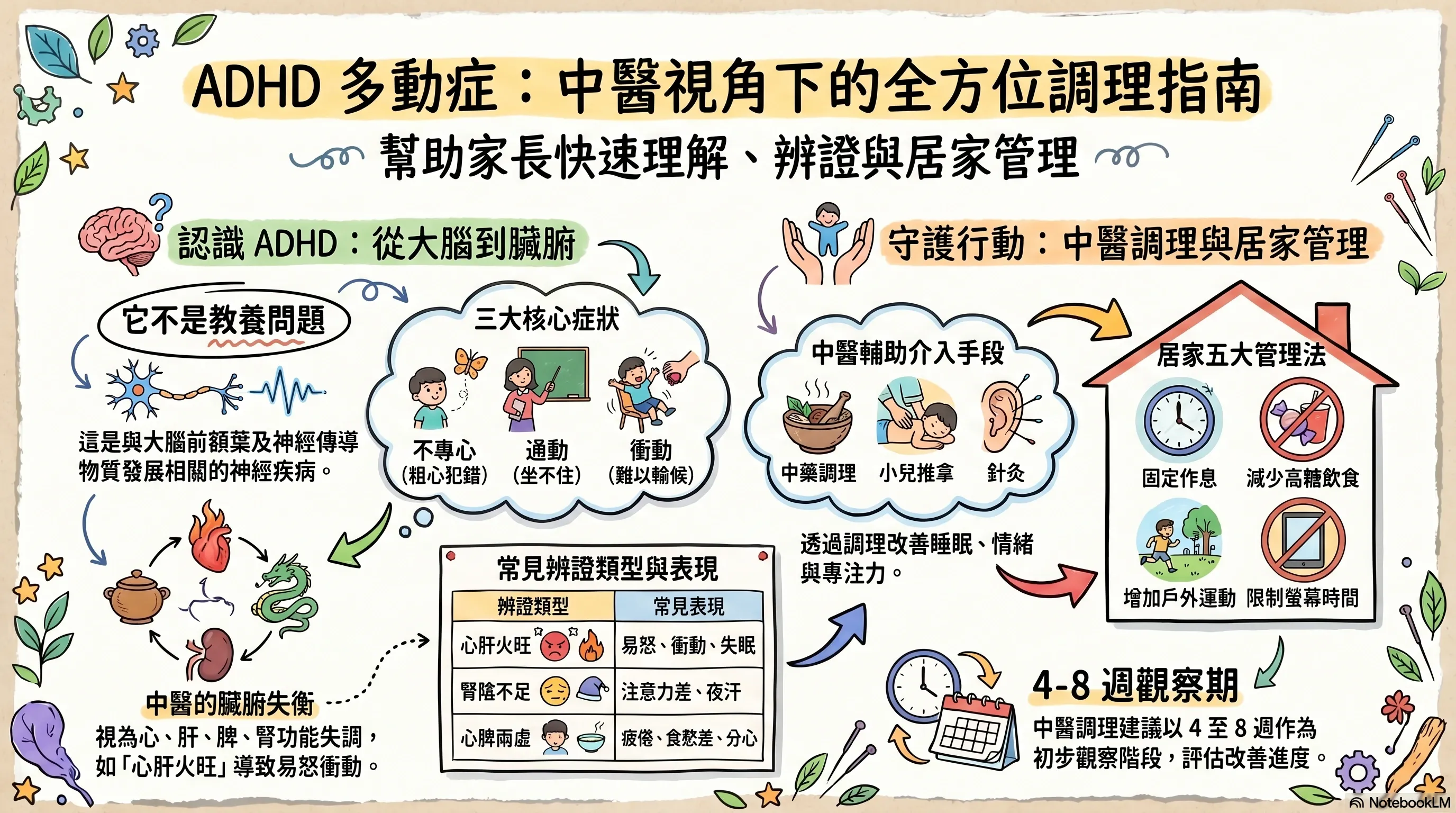
"My son cannot sit still in class — the teacher keeps complaining." "She's clearly bright, but her homework is full of careless mistakes." "He starts everything with enthusiasm but never finishes anything." Many parents quietly wonder: is this 'just lively', or could it be ADHD?
Attention Deficit Hyperactivity Disorder (ADHD) is one of the most common neurodevelopmental conditions in childhood, with a global prevalence around 5–7% and estimates in Hong Kong primary-school populations of about 5–9%. It is not a parenting issue — it is a neurodevelopmental condition linked to the prefrontal cortex and neurotransmitter systems (dopamine, noradrenaline). Diagnosis must come from a developmental paediatrician or a child psychiatrist, drawing on parent, school and psychometric information together.
Position statement: This article discusses TCM as a supportive layer of care. TCM does not replace the mainstream treatment of ADHD (behavioural therapy, school accommodations, and medication when appropriate). The TCM role is to support constitution and related symptoms — sleep, mood, digestion, attentional steadiness — so that mainstream treatment can land more effectively.
1. What Is ADHD? Diagnostic Criteria, Symptom Categories and the Three Presentations
Five Core Diagnostic Criteria
ADHD must be diagnosed by a developmental paediatrician or child psychiatrist. Following the American Psychiatric Association's DSM-5, five points are typically confirmed:
- Onset before age 12 — the pattern must have been present in childhood
- Duration of at least 6 months of inattention and/or hyperactivity-impulsivity
- Symptoms in at least two settings (such as home and school, or school and social life) — not confined to one environment
- Real functional impact on daily life, school performance or relationships
- Not better explained by another condition — anxiety, depression, sleep problems, hearing or vision issues, thyroid disease and others must be excluded
Three Symptom Categories
The presentation falls into three categories, in different proportions for each child:
Inattention
- Frequent careless mistakes; missed details
- Difficulty sustaining attention (drifting off while listening or reading)
- Trouble following through; tasks left unfinished
- Forgets daily routines; loses items (keys, books, toys)
- Avoids tasks requiring sustained mental effort
Hyperactivity
- Cannot sit still; fidgeting, tapping, squirming
- Leaves the seat when expected to stay seated
- Cannot play quietly
- Talks excessively
Impulsivity
- Difficulty waiting turns or queuing
- Blurts out answers before questions are finished
- Acts without thinking through consequences
- Interrupts conversations or activities
Three Diagnostic Presentations
Based on which categories dominate, DSM-5 recognises three presentations:
| Presentation | Main features |
|---|---|
| Predominantly inattentive | Inattention dominates; hyperactivity-impulsivity less prominent |
| Predominantly hyperactive-impulsive | Hyperactivity and impulsivity dominate; attention problems less prominent |
| Combined | Both clusters meet criteria — the most common in clinic |
Worth noting:
- ADHD in girls is often missed — girls tend to show less overt hyperactivity, presenting instead as "daydreaming" or "careless", which is why diagnosis often comes later than in boys
- Lively versus ADHD: lively children can sustain age-appropriate attention on things they enjoy; ADHD children often cannot maintain expected attention even on enjoyable tasks, with a clear gap in hyperactivity control compared with peers
- ADHD frequently co-exists with learning disorders, anxiety, mood symptoms, tic disorders (Tourette's), autism spectrum and sleep problems
2. Who Should Diagnose
ADHD is not a "I think he probably has it" decision. The standard pathway involves:
| Professional | Role |
|---|---|
| Developmental paediatrician / child psychiatrist | Primary diagnostician; integrates history, parent and teacher rating scales (SNAP-IV, Conners), developmental history |
| Clinical psychologist | Cognitive and attention testing, learning assessment, comorbidity work |
| Educational psychologist | Academic performance assessment, special educational needs profile |
| Occupational therapist | Sensory integration and executive-function assessment |
| Speech therapist | Language development if a co-occurring concern |
Important rule-outs. ADHD-like symptoms overlap with several other conditions; before diagnosis, the following should be excluded:
- Hearing or vision problems — being unable to hear or see clearly looks like "inattention"
- Thyroid disease — hyperthyroidism mimics hyperactivity; hypothyroidism slows responses
- Sleep apnoea / chronic sleep deprivation — daytime presentations can be indistinguishable from ADHD
- Mood or anxiety conditions — in children, these can present as attentional problems or restlessness
- Lead exposure, anaemia, iron deficiency — uncommon but possible contributors
3. Western Treatment: Behavioural Therapy First, Medication When Needed
Strategies vary by age and severity:
| Age / situation | Mainstream approach |
|---|---|
| Under 6 | Behavioural therapy first (parent training, behaviour management); medication not first-line |
| 6 and above, moderate-to-severe impact | Behavioural therapy plus medication (methylphenidate, atomoxetine, etc.) |
| School support | Individualised Education Plan (IEP), seating, chunked tasks, visual cues |
| Family support | Structured routines, clear instructions, positive reinforcement, parental stress management |
Medication choice and dosing must be set by a developmental paediatrician or child psychiatrist with regular review for side effects (appetite, sleep, mood, cardiovascular). TCM does not recommend stopping or reducing medication on the parent's own.
4. The TCM View: Four Pattern Directions
Classical TCM texts describe restlessness, mood instability, "forgetfulness" and "fright" under various headings ("zang zao", palpitations, "fright wind"). In clinic, four pattern directions are most commonly seen in children with ADHD:
| Pattern | Common features | Direction |
|---|---|---|
| Heart-liver fire | Marked hyperactivity, irritability, impulsivity, difficulty falling asleep, vivid dreams, halitosis, constipation, flushed face | Clear heart and liver fire, calm the spirit |
| Kidney-yin deficiency | Poor concentration, restless, slim build, frequent night urination, night sweats, warm palms and soles, easy fatigue | Nourish kidney-yin, settle the spirit |
| Heart-spleen deficiency | Poor concentration, easy fatigue, pale complexion, frequent colds, poor appetite, restless sleep | Tonify qi, strengthen spleen, nourish the heart |
| Phlegm-damp disturbance | Can't sit still, sticky mouth, thick greasy tongue coating, binge or picky eating, sluggish bowels, slower mental gear | Resolve phlegm-damp, open the senses |
In plainer language: "heart-liver fire" describes an over-excited nervous system under emotional pressure; "kidney-yin deficiency" describes weak nourishment for the brain; "heart-spleen deficiency" describes both energy supply and mood regulation running low; "phlegm-damp disturbance" describes accumulated metabolic byproducts dulling clear thinking.
Pattern differentiation must be done by a registered TCM practitioner from tongue, pulse, temperament, sleep, bowels and developmental history. Most children present with more than one pattern in combination.
5. TCM Care: Working in Support, Not in Place of, Mainstream Treatment
TCM in ADHD is supportive, not primary. The aim is to improve constitution and co-existing symptoms so mainstream treatment can work better. Common tools:
Herbal medicine. Selected by pattern. Granule or powder forms are generally chosen; a small amount of honey (over age 3) or maltose can soften the taste. One observation cycle is typically four to eight weeks. Common directions: clear heart-liver fire, nourish kidney-yin, nourish heart-blood, resolve phlegm and open the senses.
Acupuncture. Older children (over 6, cooperative) may consider acupuncture; common points include Sishencong, Shenmen, Taichong, Zusanli, Sanyinjiao. Scalp acupuncture can be helpful for attentional steadiness in some children. If the child resists needles, alternatives include ear-seed pressure, gentle gua sha and moxibustion.
Paediatric tuina. A first-line choice for younger or needle-averse children. Common techniques: clearing the heart and liver channels, kneading Taichong, spine pinching, kneading Baihui, pressing Shenmen. Parents can be taught and practise daily at home.
Lifestyle and mood guidance. Aligned with mainstream behavioural therapy — regular sleep, structured routines, reducing sugar and ultra-processed food, daily outdoor activity, limiting screen time.
Pace: four to eight weeks is one observation cycle. Objective markers include sleep duration and depth, sleep onset, morning mood, classroom feedback, school rating-scale scores, home behaviour. Any objective change should be shared with the treating paediatrician.
6. Five Things Parents Can Start Today
Even before a TCM consultation, every parent of an ADHD child can begin with:
- Sleep first. School-aged children need 9–11 hours. Sleep loss markedly worsens ADHD symptoms. Set fixed bed and wake times, with no more than an hour's drift on weekends.
- Cut sugar and ultra-processed food. High sugar and certain artificial colourings worsen hyperactive symptoms in some sensitive children. Watch behaviour 1–2 hours after sugar.
- Limit screen time. Under an hour daily, none in the hour before sleep. Fast-paced screens make attention training harder.
- 60 minutes of outdoor activity daily. Running, cycling, swimming, ball sports — any moderate-or-above activity has strong evidence for mood and attention in ADHD children.
- Structured routine plus visual cues. Use picture cards or a calendar to show "what comes next" instead of repeating verbal instructions. Pair completion with simple positive feedback.
7. Warning Signs — When Western Care Must Come First
The following situations require child-psychiatry or developmental-paediatric evaluation first:
- No formal diagnosis from a developmental paediatrician / child psychiatrist — do not start any Chinese or Western medication based only on family or teacher impressions
- Severe co-occurring mood symptoms: persistent low mood for more than two weeks, thoughts of self-harm, severe anxiety, hallucinations or disorganised speech
- A sudden behavioural deterioration in a previously stable child — withdrawal, sharp drop in school performance
- Significant side effects on ADHD medication (severe appetite loss, rapid weight drop, severe insomnia, marked mood swings, cardiovascular concerns)
- Suspected sleep apnoea (loud snoring, observed apnoea, severe daytime fatigue)
- Severe academic, social or family impact
TCM does not replace psychiatric diagnosis or medication. If ADHD is suspected but unconfirmed, the first step is a developmental paediatrician or child psychiatrist — not TCM.
8. How Western and TCM Care Work Together
| Situation | TCM role |
|---|---|
| Under 6, not on medication | Herbs and paediatric tuina alongside behavioural therapy, as early support |
| On methylphenidate / atomoxetine | Manage side effects (appetite, sleep, mood), support constitution |
| Holidays / drug holidays | TCM can strengthen constitutional work in short windows, with the prescribing doctor's agreement |
| During behavioural therapy | TCM focuses on sleep, emotional steadiness and digestion, so behavioural training takes more easily |
| Comorbidities (anxiety, tics, sleep problems) | TCM has clinical experience with co-existing mood and sleep issues |
Core principle: any change to ADHD medication is made by the developmental paediatrician or child psychiatrist — TCM does not advise families to stop, reduce or switch medication on their own.
9. How Aspira TCM Clinic Assesses
Before the first visit, parents are encouraged to bring:
- The formal diagnosis report (developmental paediatrician / child psychiatrist)
- Teacher notes or rating scales (SNAP-IV, Conners)
- Clinical psychology assessment (if available)
- Current medication list (drug, dose, start date, side-effect notes)
- Six months of sleep notes (timing, quality, night wakings, sleep talking, teeth-grinding)
- Diet log (a week of intake, snacks, sugary drinks)
- Developmental and medical history (milestones, illness frequency, birth history)
Dr To brings tongue, pulse, temperament, sleep and digestive findings together with the parents and:
- Sets out clearly which symptoms TCM may help with and which need the paediatrician's lead
- Keeps the paediatrician or psychiatrist informed (written notes on the herbal direction, passed on via parents)
- Will not advise families to stop or reduce medication on their own
An observation cycle is typically four to eight weeks.
— Dr To | Registered Chinese Medicine Practitioner (Gynaecology, TCM Aesthetics, Postpartum Belly Binding, Paediatrics) Reg. No.: 009330 Aspira TCM Clinic
Frequently Asked Questions
Q1: Can TCM replace methylphenidate (Ritalin, Concerta)?
No. Methylphenidate is a prescription medication initiated by a developmental paediatrician or child psychiatrist. There is no clinical evidence that TCM can replace its effects. The TCM role is supportive: improving co-existing sleep, mood and digestive issues, and managing side effects. Any decision to stop or reduce medication rests with the prescribing doctor.
Q2: Can Chinese herbs clash with ADHD medication?
In theory, yes. Some herbs (such as ephedra, ginseng, strongly stimulating or yang-tonic preparations) may influence neural excitability and could stack with stimulants (methylphenidate). Tell the TCM practitioner exactly which ADHD medication your child is on, the dose and the dosing schedule — a registered TCM practitioner will choose a relatively mild direction that does not compound stimulation.
Q3: My child is very active but school hasn't raised concerns — do we need an assessment?
"Lively" is not the same as ADHD. The diagnostic threshold requires functional impact in two or more settings (home, school, social). If your child:
- Performs at age level academically
- Has good peer relationships
- Manages emotions reasonably
- Can sustain attention for 15–20 minutes on tasks they choose
then "active" generally does not need a medical workup. If concerns persist, school feedback shifts, academic performance drops or the gap with peers becomes obvious, start with a developmental paediatrician.
Q4: My child won't accept acupuncture — what now?
Options include: (1) paediatric tuina (no needles; parents can be taught); (2) ear-seed pressure (vaccaria seeds taped on ear points, painless); (3) scalp acupuncture with brief needle retention (for cooperative children over 6); (4) moxibustion or acupressure. TCM tools extend beyond acupuncture, and Dr To selects the right format based on the child's age and temperament.
Q5: Will ADHD "go away with age"?
Some symptoms (especially overt hyperactivity) often decrease with age — but around 50–65% of patients continue to have attention and executive-function difficulties into adulthood, affecting work, relationships and mood. Early intervention (behavioural therapy, school accommodations, medication when appropriate, and TCM support) helps reduce long-term impact and build coping skills. "He'll grow out of it" is not a reliable strategy.
Already Diagnosed with ADHD and Looking for TCM Support? Book a Consultation
If your child has a confirmed ADHD diagnosis from a developmental paediatrician or child psychiatrist and you would like TCM support for constitution, sleep, mood or medication side effects, please bring the formal diagnosis report, school rating scales, current medication list and sleep / diet notes before booking a consultation with Dr To. For children without a formal diagnosis, please see a developmental paediatrician or child psychiatrist first.
How to book:
- WhatsApp: Book here
- Phone: 2110 9337
- Address: Unit 2706, 27/F, Saxon Tower, 7 Cheung Shun Street, Lai Chi Kok
Disclaimer: This article is for general health education only and does not replace individual diagnosis, examination, medication or treatment advice. ADHD is a neurodevelopmental condition that must be diagnosed and led by a developmental paediatrician or child psychiatrist. Children differ in constitution; specific TCM plans should be discussed with a registered TCM practitioner. Any change to ADHD medication must first be discussed with the prescribing doctor.
Disclaimer: This article is for health education and reference purposes only and does not constitute medical advice, diagnosis, or treatment. Each patient's condition is unique and treatment outcomes vary. Please consult a registered TCM practitioner or qualified healthcare professional for health concerns.
Further Reading
Hand-picked related articles and real cases to read next.
Kids Won't Eat? A TCM Perspective on the Causes and What Parents Can Do
Poor appetite in children is one of the most common parenting headaches. This article breaks down four common causes from a TCM perspective (spleen-stomach weakness, food retention, liver stagnation, post-viral effects), three things parents can start today, five common paediatric tuina techniques, three gentle food therapies, and the warning signs that warrant a paediatrician first.
TCM Limitations: 5 Times to See a Western Doctor First
TCM has genuine strengths in chronic care and holistic wellness, but it is not the right first choice for every situation. This article honestly discusses 5 scenarios where Western medicine should come first, what TCM truly excels at, and how to make informed decisions between the two.
TCM vs Western Medicine: 6 Common Conditions Compared
Is TCM or Western medicine better? The honest answer: it depends on your condition and needs. This article fairly compares both approaches across six common conditions — cough, eczema, pain, insomnia, digestive issues, and menstrual irregularities — to help you make the right choice.
Want to learn more? WhatsApp us for a free consultation
Book via WhatsAppExplore our full range of treatments: Traditional TCM Services
Related Articles

Do Oysters, Maca and Deer Antler Boost Male Vitality? 5 Myths
Do aphrodisiac foods actually work? This article opens with a rating table (effective / partly effective / effective within a TCM framework / weak evidence / no strong evidence), reviews the Chinese and Western medical evidence behind oysters, maca, deer antler, sea cucumber and Chinese chives, distils the 3 shared traits of foods that genuinely support male sexual function, and flags 3 commonly eaten items that can actually harm performance.

Male Menopause Through the TCM Lens: 5 Signs in Men Over 40
Unexplained fatigue, irritability, lower libido, poorer sleep and a growing belly after 40 are not just ageing or work stress — they may be male menopause. This article begins with a five-sign self-check, sets out three TCM patterns (kidney-yang deficiency, kidney-yin deficiency, liver-and-kidney insufficiency) with matching improvements, and compares the two treatment routes — testosterone replacement therapy versus TCM constitutional care.
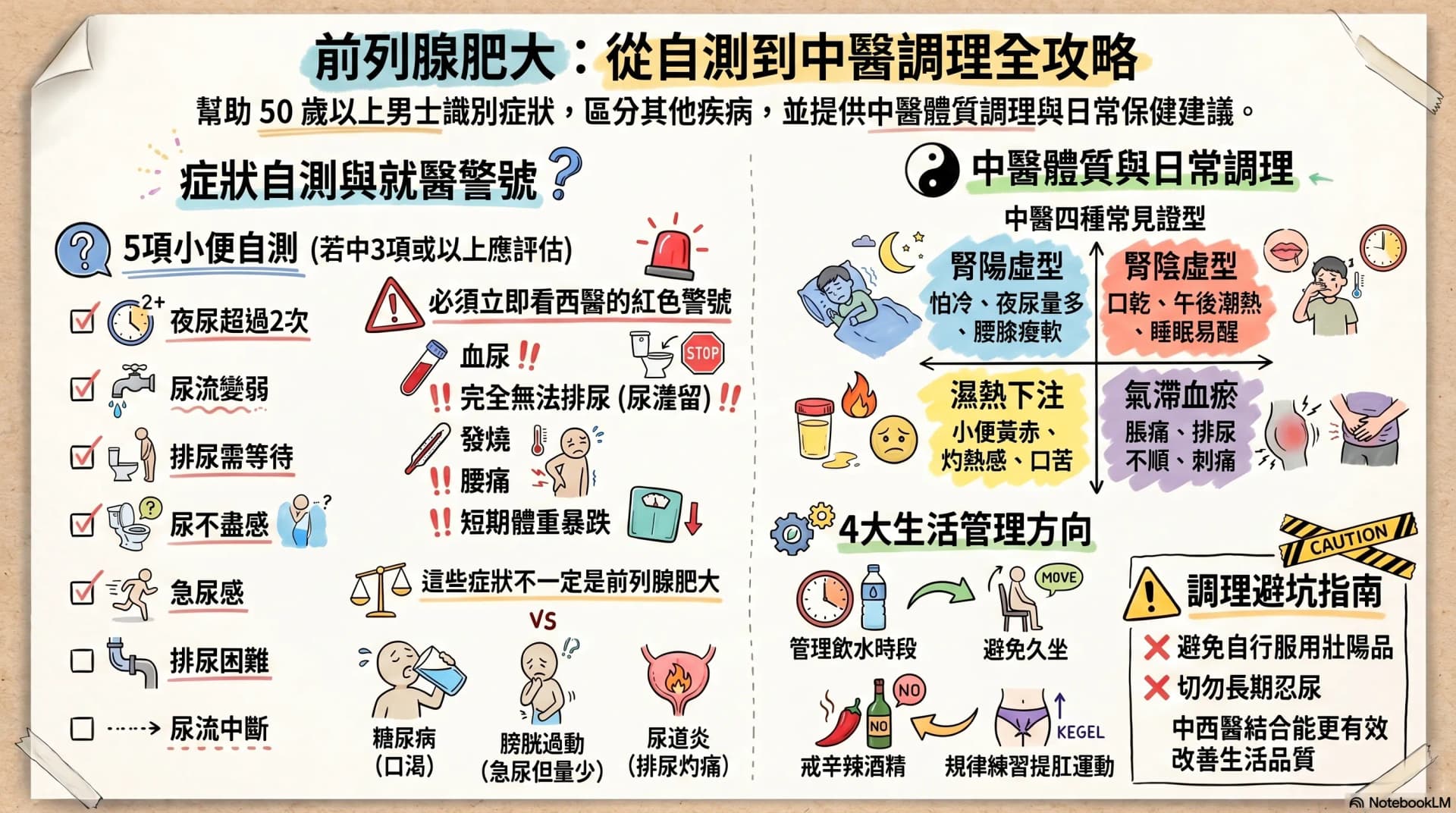
Enlarged Prostate: Are Nocturia and a Weak Stream Warning Signs?
After age 50, urinary frequency, nocturia, a weaker stream and having to urinate in stages may not simply be ageing. This article opens with a 7-symptom self-check, then sets out warning signs that warrant seeing a Western doctor immediately, four TCM constitution patterns, and four daily care directions any man can start with — helping you or your father decide the next step.