Slim Women Get PCOS / PMOS Too — Recognising and Managing PCOS in Lean Patients
A normal BMI does not rule out PCOS / PMOS. Lean PCOS accounts for around 20–30% of patients — insulin resistance, hyperandrogenism and irregular cycles are all still in play, but the diagnosis is routinely missed because the patient is not overweight. This article walks through the comparison with the classic phenotype, five recognition signals, the necessary investigations, three common TCM pattern directions and why the lean phenotype is managed differently.
Medical review: Dr. Chan Wing Kiu, Joanne,Registered Chinese Medicine Practitioner #009463
1-Minute Quick Answer
A normal BMI does not rule out PCOS / PMOS; lean PCOS is around 20-30% of patients, with insulin resistance, hyperandrogenism and irregular cycles still in play but easily missed. Recognition cues include scanty periods, acne, hair growth and marked post-meal fatigue. Care focuses on blood-sugar stability, not weight loss; amenorrhoea over six months needs a gynaecological workup first.
Slim Women Get PCOS / PMOS Too — Recognising and Managing PCOS in Lean Patients
 For quick reference, this image was generated by NotebookLM. Some Chinese characters may not render perfectly; we appreciate your understanding.
For quick reference, this image was generated by NotebookLM. Some Chinese characters may not render perfectly; we appreciate your understanding.
Medical review: Dr Chan (CMCHK 009463 | Geriatric gynaecology, perimenopause, uterine fibroids, internal medicine)
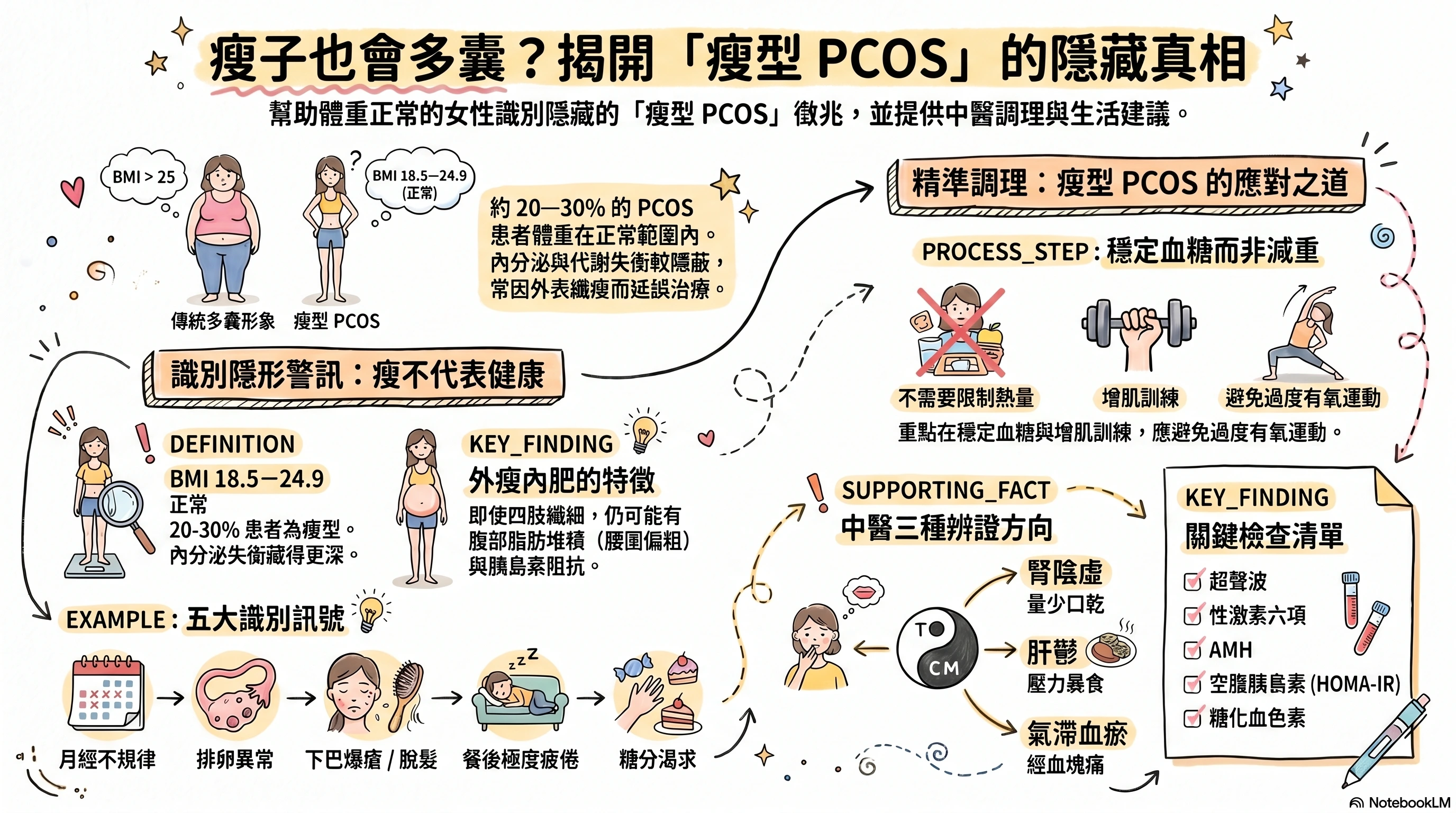
"I'm not even heavy — how could I possibly have polycystic ovary syndrome?" This is the first thing many slim women say when they hear the diagnosis of PCOS (now renamed PMOS — Polyendocrine Metabolic Ovarian Syndrome by the 2026 expert consensus in The Lancet). In reality, around 20–30% of PCOS / PMOS patients have a BMI within the normal range — a presentation clinicians call "lean PCOS". Their insulin resistance, hyperandrogenism, and ovulatory disturbance do not disappear because they are slim — and the diagnosis is often delayed precisely because they "don't look the part".
This article walks through the comparison with the classic phenotype, five recognition signals, the investigations to ask for, three common TCM pattern directions, and why lean PCOS is managed differently from the classic phenotype.
1. Lean vs Classic PCOS — A Comparison
| Item | Lean PCOS | Classic PCOS |
|---|---|---|
| BMI | Normal (18.5–24.9) | Raised (≥ 25) |
| Insulin resistance | Present but milder and more covert | More pronounced |
| Hyperandrogenism | May be milder, but acne, hair growth and hair thinning still occur | More pronounced |
| Menstrual irregularity | Equally common | Equally common |
| Waist-to-hip ratio | Even when slim, waist may be relatively wide (higher visceral fat) | Higher overall body fat |
| Recognition cues | Cycle, androgenic symptoms, post-meal fatigue | Weight, waist, acanthosis nigricans |
| Care emphasis | Blood-sugar stability, cycle regulation, kidney and liver work | Weight reduction, improving insulin resistance, resolving phlegm-damp |
Key idea: lean PCOS is not "a lighter version" of PCOS. The endocrine and metabolic imbalance is just as real — it is simply better hidden. Long-term neglect carries the same risks: endometrial hyperplasia, diabetes and cardiovascular disease.
2. Five Recognition Signals for Lean PCOS
A normal BMI plus two to three or more of the following warrants a gynaecological or endocrine workup:
- Irregular cycles or amenorrhoea — cycles longer than 35 days, fewer than 8 periods a year, or amenorrhoea
- Irregular ovulation — basal body temperature charts that look monophasic or unclear; ovulation tests rarely catch a clear surge
- Androgenic symptoms — despite being slim: recurrent jawline acne, upper-lip hair, marked thinning at the crown (male-pattern hair loss)
- Marked post-meal fatigue and sugar cravings — feeling deeply sleepy or craving sweets 1–2 hours after meals — a clue to covert insulin resistance
- Wider waist or noticeable abdominal fat — even with a normal overall body, waist ≥ 80 cm or waist-to-hip ratio ≥ 0.85 — a clue to higher visceral fat
Worth noting: the absence of acanthosis nigricans does not mean there is no insulin resistance. Acanthosis appears mainly with more severe insulin resistance; in lean PCOS the resistance is often subtler and skin changes may be absent altogether.
3. Why Lean PCOS Is Easily Missed
- Stereotyped image: many people equate PCOS with obesity, hirsutism and irregular periods — the first criterion is missing in lean PCOS
- Lower clinical suspicion: those with a normal BMI are less often screened for metabolic risk
- Ultrasound findings: some lean PCOS cases do not show the classic "string of pearls", making imaging less helpful
- Patient perception: feeling "not heavy, probably fine" delays seeking help
- Milder external signs: acne and hair growth in lean PCOS can be subtle and dismissed as "personal constitution"
This is one of the reasons the 2026 expert consensus in The Lancet renamed PCOS to PMOS (Polycystic Metabolic Ovarian Syndrome) — to emphasise the metabolic core and remind clinicians not to rely on body weight as the gatekeeper for diagnosis.
4. The TCM View: Three Pattern Directions for Lean PCOS
The classic-phenotype PCOS in TCM revolves around "spleen deficiency with phlegm-damp". The lean phenotype tends to centre on three different directions:
| Pattern | Common features | Direction |
|---|---|---|
| Kidney-yin deficiency | Scanty periods or amenorrhoea, hot flushes, dry mouth, night thirst, warm palms and soles, thinning hair, dry skin | Nourish kidney-yin, build blood, regulate the cycle |
| Liver-qi stagnation (stress-binge type) | Irregular cycles, premenstrual chest and breast tension, difficulty sleeping, jawline acne, stress-related binging on sweets | Soothe the liver, regulate qi, clear liver heat |
| Qi-blood stagnation | Scanty periods with clots, premenstrual stabbing lower-abdominal pain, dusky tongue edges | Move qi and blood, regulate the cycle |
Lean PCOS patients frequently present with overlapping patterns (for example, "kidney-yin deficiency with liver-qi stagnation" or "liver stagnation generating heat with blood stasis"). Prescriptions are decided by a registered TCM practitioner using tongue and pulse, menstrual history and recent investigations.
In simpler terms: "kidney-yin deficiency" describes a body running short on its restorative and reproductive baseline; "liver-qi stagnation" describes qi and mood stuck under pressure; "qi-blood stagnation" describes both flow systems running rough.
5. Lean PCOS Is Managed Differently
For classic PCOS, "lose 5–10%" is often the first recommendation. For lean PCOS, weight loss is neither necessary nor helpful. The priorities shift:
| Domain | Lean PCOS approach |
|---|---|
| Diet | Not a calorie cut — a blood-sugar focus: low-GI, more protein and fibre, no fasted sweet drinks; small frequent meals often outperform long fasting |
| Exercise | Muscle-building first (resistance training 2–3 times a week) to improve insulin sensitivity; avoid excessive cardio that may aggravate amenorrhoea |
| Sleep | Sleep before 11 pm, seven or more hours a night |
| Stress management | Especially important for liver-stagnation type — meditation, yoga, steady hobbies |
| Herbs | Mostly kidney-tonifying, liver-soothing, cycle-regulating; less emphasis on heavy spleen-and-phlegm work (which suits the classic phenotype better) |
| Western adjuncts | The COCP may protect the endometrium and regulate cycles; ovulation induction when fertility is the goal; metformin less commonly first-line, but considered when insulin resistance is documented |
Key principle: lean PCOS is not "if I just get a bit thinner it'll resolve". Over-restriction can layer on functional hypothalamic amenorrhoea and make cycles worse. The diet emphasis is quality and structure, not calorie deficit.
6. Investigations to Ask For
A common reason lean PCOS is missed is that metabolic markers are not actively checked. If two to three or more of the recognition signals fit, request the following workup:
- Reproductive hormones (FSH, LH, E2, PRL, testosterone, progesterone)
- AMH (anti-Müllerian hormone)
- Fasting insulin plus HOMA-IR (the key for covert insulin resistance — often not ordered for normal-BMI patients)
- Fasting glucose plus HbA1c
- Thyroid function, prolactin (to exclude other endocrine causes)
- Pelvic ultrasound
7. Warning Signs Requiring Western Evaluation First
- Sudden marked weight loss or gain, severe hirsutism, voice deepening or noticeable muscle gain — to rule out other endocrine conditions
- Amenorrhoea for more than six months (not pregnant, not breastfeeding)
- Trying to conceive for over 12 months (or 6 months if over 35) without success
- Severe mood symptoms or a binge–restrict cycle
8. How Aspira TCM Clinic Assesses Lean PCOS
Before the first visit, please bring:
- A menstrual cycle log over the past year
- Recent gynaecological reports (ultrasound, hormones, AMH, fasting insulin)
- Weight, waist and body-composition history
- A current medication and supplement list
- An outline of diet, exercise and sleep habits
- Any pregnancy plans
Dr Chan tailors the programme to pattern, cycle phase and fertility goals, and:
- Keeps the gynaecologist or endocrinologist informed (written notes on the herbal direction, passed via the patient)
- Does not recommend over-restriction, focusing instead on blood-sugar stability, cycle regularity and constitution
- Provides concrete diet, exercise and sleep recommendations alongside
— Dr Chan Wing Kiu | Registered Chinese Medicine Practitioner (Geriatric Gynaecology, Internal Medicine) Reg. No.: 009463 Aspira TCM Clinic
Frequently Asked Questions
Q1: My BMI is 21 and my cycle runs 35–40 days — could this be lean PCOS?
Possibly. A cycle of 35 days or more falls into the "oligo-ovulation" range, meeting one of the PCOS criteria. A workup with reproductive hormones, AMH, fasting insulin plus HOMA-IR and pelvic ultrasound is worth arranging with a gynaecologist.
Q2: Is lean PCOS harder to conceive with than the classic phenotype?
Not necessarily. Conception probability depends more on ovulatory regularity and egg quality than on body weight. For lean PCOS, the priority is restoring regular ovulation — cycle-based TCM care alongside ovulation tracking or induction medication has helped many lean PCOS patients conceive naturally.
Q3: Can lean PCOS slowly "turn into" classic PCOS?
It can. With age (metabolic rate falls after 30) and life changes (stress, eating out, less exercise), insulin resistance can worsen, weight can rise, and the picture can shift toward the classic phenotype. Earlier recognition and intervention give more protection.
Q4: Is basal body temperature charting useful, and how is it done?
Especially useful for lean PCOS — it helps determine whether ovulation is happening. Method: every morning, before getting up, use a basal thermometer (accurate to 0.05°C) under the tongue, charting through one full cycle. Regular ovulation shows a biphasic pattern (low follicular phase, higher luteal phase by 0.3–0.5°C); anovulation shows a flat monophasic line.
Q5: I'm slim but have acne and hair growth — should I stop all skincare?
No. The priority is identifying the endocrine cause (hormones, AMH, cortisol) — is this androgenic, adrenal, or something else? Gentle skincare can continue; avoid harsh exfoliation and overly stripping products. If acne has persisted for over six months alongside menstrual irregularity, a joint workup by gynaecology and dermatology, with TCM care alongside, is the most useful approach.
Wondering if You Have Lean PCOS? Book a Consultation
If your BMI is normal but you have menstrual irregularity, acne, hair growth or marked post-meal fatigue, please bring your gynaecological report (including fasting insulin + HOMA-IR), menstrual log and basal temperature chart (if any) before booking a consultation with Dr Chan. Any medication change should first be discussed with your gynaecologist.
How to book:
- WhatsApp: Book here
- Phone: 2110 9337
- Address: Unit 2706, 27/F, Saxon Tower, 7 Cheung Shun Street, Lai Chi Kok
Disclaimer: This article is for general health education only and does not replace individual diagnosis, examination, medication or treatment advice. Lean PCOS is a long-term endocrine and metabolic condition; treatment plans must be individualised and built jointly by a gynaecologist or endocrinologist and a registered TCM practitioner. Any change to oral contraceptives, metformin or ovulation-induction medications must first be discussed with the prescribing doctor.
References
- The Lancet (2026) — Expert consensus on renaming PCOS to PMOS (Polyendocrine Metabolic Ovarian Syndrome). https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(26)00717-8/fulltext
Disclaimer: This article is for health education and reference purposes only and does not constitute medical advice, diagnosis, or treatment. Each patient's condition is unique and treatment outcomes vary. Please consult a registered TCM practitioner or qualified healthcare professional for health concerns.
Further Reading
Hand-picked related articles and real cases to read next.
PCOS Renamed PMOS — Symptom Self-Check and Combined Western–TCM Care
PCOS has been renamed PMOS (Polyendocrine Metabolic Ovarian Syndrome) to emphasise that it is not only a gynaecological condition but a metabolic one. This article walks through how PMOS develops (Western and TCM views), a three-category nine-point symptom self-check, the combined Western–TCM treatment plan, and practical low-GI diet and resistance-training steps every patient can start at home.
Polycystic Ovary Syndrome (PCOS): Causes and TCM Care for Menstrual Irregularity, Hair Growth, Acne and Infertility
PCOS is not simply "irregular periods" — it is a long-term condition spanning the endocrine, metabolic and reproductive axes. This article covers common symptoms, four TCM pattern directions (kidney deficiency, phlegm-damp, liver stagnation, qi-blood stagnation), TCM care (cycle-based therapy, acupuncture, weight and insulin resistance management), how to coordinate with Western treatment, and the investigations and warning signs to know.
A Self-Check Guide to 4 Types of Menstrual Pain and Relief Tips
Menstrual pain is not something you simply have to endure. This guide explains the difference between primary and secondary dysmenorrhea, outlines four common TCM patterns, highlights five warning signs that need medical review, and offers practical relief strategies for everyday care.
Want to learn more? WhatsApp us for a free consultation
Book via WhatsAppExplore our full range of treatments: Traditional TCM Services
Related Articles

Do Oysters, Maca and Deer Antler Boost Male Vitality? 5 Myths
Do aphrodisiac foods actually work? This article opens with a rating table (effective / partly effective / effective within a TCM framework / weak evidence / no strong evidence), reviews the Chinese and Western medical evidence behind oysters, maca, deer antler, sea cucumber and Chinese chives, distils the 3 shared traits of foods that genuinely support male sexual function, and flags 3 commonly eaten items that can actually harm performance.

Male Menopause Through the TCM Lens: 5 Signs in Men Over 40
Unexplained fatigue, irritability, lower libido, poorer sleep and a growing belly after 40 are not just ageing or work stress — they may be male menopause. This article begins with a five-sign self-check, sets out three TCM patterns (kidney-yang deficiency, kidney-yin deficiency, liver-and-kidney insufficiency) with matching improvements, and compares the two treatment routes — testosterone replacement therapy versus TCM constitutional care.
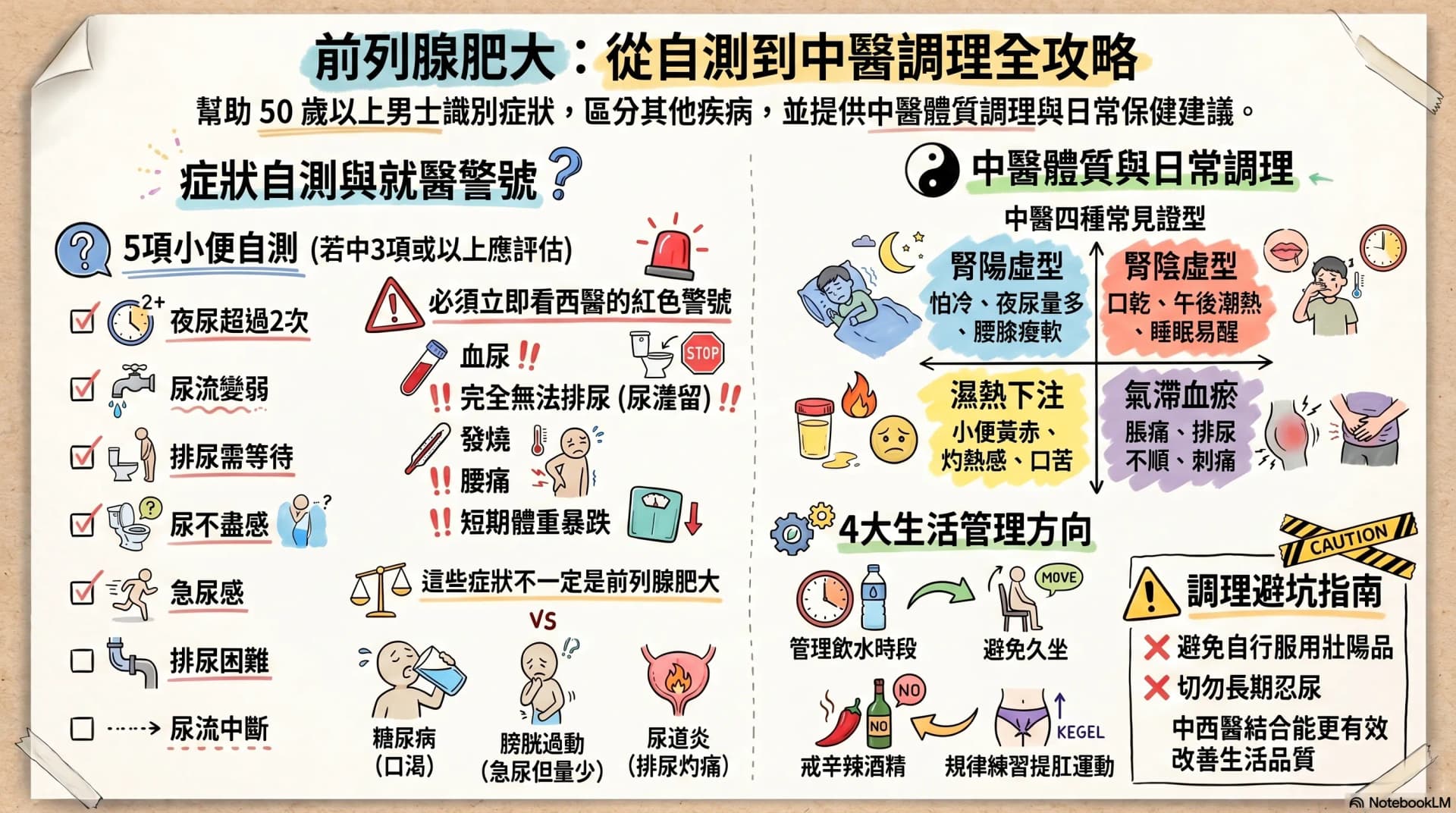
Enlarged Prostate: Are Nocturia and a Weak Stream Warning Signs?
After age 50, urinary frequency, nocturia, a weaker stream and having to urinate in stages may not simply be ageing. This article opens with a 7-symptom self-check, then sets out warning signs that warrant seeing a Western doctor immediately, four TCM constitution patterns, and four daily care directions any man can start with — helping you or your father decide the next step.